![]()
Part 1
Principles of Research in Healthcare
![]()
1 Evidence-Based Practice and Research
Jo Rycroft-Malone
DEFINITION
The concern with providing patients with the best and safest care possible is often referred to as evidence-based practice. Evidence-based practice has been defined as the combination of research, clinical experience, local information and patients’ preferences and experience in the delivery of care and services (Rycroft-Malone et al., 2004a). Evidence-based practice has become a policy imperative in many countries, with an associated investment in guideline development bodies, such as the National Institute for Health and Clinical Excellence (NICE, www.nice.org.uk), to support practitioners, plus services deliver on this agenda. Despite this focus and investment, there are many examples of patients receiving treatment, care and interventions that are known to be less than effective and even harmful.
There are many challenges to using evidence in practice. While practitioners genuinely wish to do the right thing for patients, robust research is just one of several components that inform health professionals in their everyday practice and many factors influence this process. The Promoting Action on Research Implementation in Health Services (PARIHS) framework provides a way of thinking about how some of these challenges can be identified and considered.
KEY POINTS
• The PARIHS framework was developed in an attempt to reflect the interdependence and interplay of the many factors that appear to play a role in the successful implementation of evidence in practice. It was developed inductively and has been refined over time (see Rycroft-Malone, 2010 and Kitson et al., 2008 for a summary)
• Successful implementation is represented as a function of the nature of evidence, the quality of the context of implementation and appropriate approaches to facilitation. This relationship is represented as: SI = f (E, C, F) – that is, successful implementation = function (evidence, context, facilitation)
• Evidence, context and facilitation are each positioned on a ‘high’ to ‘low’ continuum. Moving towards the high end of the continuum increases the chances of successful implementation of evidence-based practice (Rycroft-Malone et al., 2004b)
• The proposition is that evidence-based practice is most likely to occur when evidence is scientifically robust and matches a professional consensus, patients’ experiences and preferences and is informed by local information/data (‘high’ evidence), the context is receptive to change with appropriate cultures, leadership and robust monitoring and feedback systems (‘high’ context) and when there is appropriate support for change with input from skilled external and/or internal facilitators (‘high’ facilitation)
• The PARIHS framework should be useful for understanding some of the key ingredients of evidence-based practice, guiding evidence-based practice and as an aide-memoire in practice
DISCUSSION
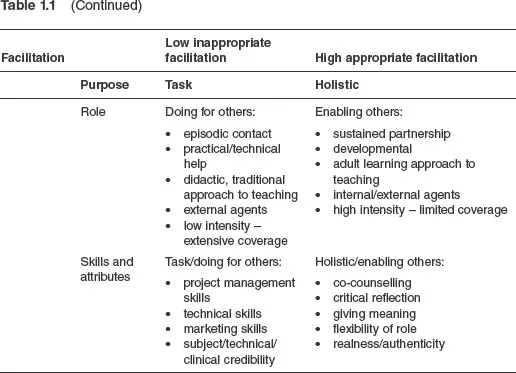
See Table 1.1 for a description of the various elements and sub-elements of the PARIHS framework.
Table 1.1Elements and sub-elements of the PARIHS framework
Evidence
Within PARIHS, evidence is conceived in a broad sense to include four different types of evidence:
• research
• clinical experience
• patients’ and carers’ experiences
• local context information (see Rycroft-Malone et al., 2004a).
These sources of evidence are blended in decision-making to make appropriate patient-centred decisions based on the best research evidence available. This process is interactive and may need to be guided by a skilled facilitator.
Context
Context refers to the environment or setting in which the proposed change is to be implemented (see McCormack et al., 2002). The quality and nature of the contexts in which we work can have a more or less facilitative influence on our ability to change and develop practices based on evidence. Within PARIHS, the contextual factors that promote successful implementation fall under three broad sub-elements that operate in a dynamic way:
• culture
• leadership
• evaluation.
Facilitation
Facilitation refers to the process of enabling or making easier the implementation of evidence in practice (see Harvey et al., 2002). Facilitation is achieved by an individual carrying out a specific role – that of being a facilitator, with the appropriate skills and knowledge to help individuals, teams and organisations use evidence in practice.
Facilitators have a key role to play in developing contexts that are conducive to the use of evidence. Part of this process is also about working with practitioners to help them make sense of evidence. The purpose, role, skills and attributes of facilitators are absolutely critical to implementing evidence-based practice.
CASE STUDY
PARIHS has been used in different ways (see Rycroft-Malone, 2010 for a summary). A number of tools and instruments have also been developed based on PARIHS. For example, the Context Assessment Index (McCormack et al., 2009) has been developed to assist practitioners with assessing and understanding the context in which they work and the effect this has on implementing evidence into practice. PARIHS has also been used with research and implementation activity as a conceptual and theoretical framework – that is, as an organising framework to underpin and/or guide evidence-based practice. For example, the elements can be used to understand or ‘diagnose’ a situation and help structure questions to make sense of situations, as follows.
Evidence
• Is there any research evidence underpinning the initiative/topic?
• Is this research judged to be well conceived, designed and conducted?
• Are the findings from research relevant to the initiative/topic?
• What is the practitioner’s experience and opinion about this topic and the research evidence?
• Does the research evidence match with clinical, organisational and facilitation experience?
• Do you need to seek consensus before it might be used by practitioners in this setting? How might you do this in your workplace?
• What is the patient’s experience/preference/story concerning this initiative/topic?
• Does this differ from practitioners’ perspectives?
• How could a partnership approach be developed?
• Is there any robust, local information/data about the initiative/topic?
Context
• Is the context of implementation receptive to change?
• What are the beliefs and values of the organisation, team and practice context?
• What sort of leadership style is present (command and control, transformational)?
• Are individual and team boundaries clear?
• Is there effective teamworking?
• Does evaluation of performance rely on broad and varied sources of information?
• Is this information fed back to clinical contexts?
Facilitation
• Consider the answers to the evidence and context questions: what are the barriers and what are the facilitators to this initiative?
• What tasks/activities and processes require facilitation?
For a comprehensive review and critique of how PARIHS has been used previously, refer to Helfrich et al. (2010).
CONCLUSION
Evidence-based practice requires individual, team and organisational effort. Using evidence in practice is complex and challenging, which goes far beyond an individual’s ability to critically appraise research. The PARIHS framework represents this complexity and provides a map of the factors that play a role and therefore need to be paid attention to in any evidence-based practice-related activities.
FURTHER READING
Rycroft-Malone, J. and Bucknall, T. (2010) Models and Frameworks for Implementing Evidence-Based Practice. Oxford: Wiley Blackwell.
Stetler, C.B., Damschroder, L.J., Helfrich, C.D. and Hagedorn, H.J. (2011) ‘A guide for applying a revised version of the PARIHS framework for implementation’, Implementation Science, 6: 99.
REFERENCES
Harvey, G., Loftus-Hills, A., Rycroft-Malone, J., Titchen, A., Kitson, A., McCormack, B. and Seers, K. (2002) ‘Getting evidence into practice: The role and function of facilitation’, Journal of Advanced Nursing, 37 (6): 577–88.
Helfrich, C.D., Damschroder, L.J., Hagedorn, H.J., Daggett, G.S., Sahay, A., Ritchie, M., Damush, T., Guihan, M., Ullrich, P.M. and Stetler, C.B. (2010) ‘A critical synthesis of literature on the promoting action on research implementation in health services (PARIHS) framework’, Implementation Science, 5: 82.
Kitson, A., Rycroft-Malone, J., Harvey, G., McCormack, B., Seers, K. and Titchen, A. (2008) ‘Evaluating the successful implementation of evidence into practice using the PARIHS framework: Theoretical and practical challenges’, Implementation Science, 3: 1.
McCormack, B., Kitson, A., Harvey, G., Rycroft-Malone, J., Titchen, A. and Seers, K. (2002) ‘Getting evidence into practice – the meaning of “context”’, Journal of Advanced Nursing, 38 (1): 94–104.
McCormack, B., McCarthy, G., Wright, J., Slater, P. and Coffey, A. (2009) ‘Development and testing of the context assessment index (CAI)’, Worldviews on Evidence-based Nursing, 6 (1): 27–35.
Rycroft-Malone, J. (2010) ‘Promoting Action on Research Implementation in Health Services Framework’, in J. Rycroft-Malone and T. Bucknall (eds), Theory and Frameworks for Implementing Evidence-Based Practice. Oxford: Wiley Blackwell. pp. 109–35.
Rycroft-Malone, J., Harvey, G., Seers, K., Kitson, A., McCormack, B. and Titchen, A. (2004a) ‘An exploration of the factors that influence the implementation of evidence into practice’, Journal of Clinical Nursing, 13: 913–24.
Rycroft-Malone, J., Seers, K.,Titchen, A., Harvey, G., Kitson, A. and McCormack, B. (2004b) ‘What counts as evidence in evidence-based practice?’, Journal of Advanced Nursing, 47 (1): 81–90.
![]()
2 Creating a Research-Based Culture in Healthcare Practice
Joyce Wilkinson
DEFINITION
Culture has been described as ‘the way things are done around here’ (Davies et al., 2000: 111). So, creating a research-based culture in healthcare practice would focus on making research a fundamental part of that, so it becomes an everyday aspect of practice. Likewise, such a culture would be one in which practice is built on research and informed by it and in which healthcare practitioners consider research when they make decisions about practice. Research-based cultures can be supported by practice development, staff development and developing research partnerships.
KEY POINTS
• Using research in practice is the cornerstone of high-quality healthcare (Parahoo, 2006) and a fundamental aspect of practice development
• Research is only one type of evidence for practice (Rycroft-Malone et al., 2004), but needs to be given consideration along with other types of information, although it may not be the first source of evidence that nurses consult (Thompson et al., 2001)
• Practice development is not only in the remit of those with specific roles but also the responsibility of all staff
• Using research in practice is broader than directly applying research findings to practice. It can also be used to improve knowledge, change attitudes and behaviour or lobby for change
• Research should form the foundation of all aspects of staff development
• Developing the capacity of individuals and teams or whole healthcare organisations to use research is at least as important as teaching staff about how to do research
• It is not necessary for all staff to have research skills as it can be embedded into policies and procedures that staff must follow, so they use research without necessarily being aware of it
• Staff development is largely an organisational responsibility, whereas practice development is often more an individual responsibility, but individuals also have to take responsibility for making the most of opportunities for staff development
• Researchers are increasingly interested in building strong partnerships with clinical staff and organisations (Rycroft-Malone, 2012). Many of these partnerships focus on doing and using research in practice, so the two are mutually important and supportive
• Research partnerships offer opportunities for staff development and practice development, providing benefits ...