![]()
Chapter 1
Approaches to Nursing Children, Young People and their Families
Key points
• Caring for children, young people and their families requires well developed understandings of the health, psychological, developmental, communication and cultural needs of each child and young person.
• The family is an integral part of how children and young people experience and engage in society and health care.
• Family-centred care and child-centred care are key philosophies underpinning the nursing care of children and young people; however, their application in practice is not without problems.
• Children are not a homogenous group and each child has their own individual perspectives and experiences.
• Children and young people with complex care needs require special considerations to ensure their health, well-being and rights are met.
• Transitioning from paediatric to adult care settings can present issues for young people, their parents and health care professionals.
Key theories and concepts explored in this chapter are child-centred care, family-centred care, children participating in their care and transitioning between services.
Case study 1.1: Mikael
Setting the scene
Mikael is 4 years old and has just been diagnosed with type 1 diabetes mellitus. He lives with his parents, Catherine and John and his two siblings, Sarah aged 1 year and Sam aged 6 years. Mikael is an active, inquisitive child, who is ‘into everything’. The family moved to the area a couple of years ago, so do not have an extended family support network close by.
Mikael was admitted to hospital in diabetic ketoacidosis and spent two days in intensive care for initial stabilisation. He was then transferred to the children’s ward for further care and education. He spent a total of six days in hospital. The time Mikael was in intensive care was a very stressful time for the family and they also needed to come to terms with Mikael’s unexpected and new diagnosis of type 1 diabetes. Because of his young age, Mikael will be fully reliant on his parents for the monitoring and management of his diabetes, including initially six finger pricks a day to monitor blood glucose levels, insulin injections morning and evening, his diet and general well-being.
John (Mikael’s father) needed to return to work after the first three days of Mikael’s hospitalisation. He travels across town to his job and works long hours. This meant that Mikael’s mother, Catherine, was taught the skills she needed to be able to care for Mikael and she was expected to teach John these skills. Catherine stayed with Mikael for the first two nights on the children’s ward but was not able to stay for the other nights. The family only had one car and so on the last two days of his admission, Catherine and the baby travelled an hour to the hospital by bus after seeing Sam off to school. Although Catherine missed being there for Mikael’s morning insulin on these days, she was there during the day to receive education and for his evening dose of insulin. John called in to spend a short but enjoyable time with Mikael before taking Catherine and the baby home, and picking Sam up from a friend’s place along the way.
Introduction
This chapter focuses on the philosophical underpinnings of children’s and young peoples’ nursing. In the discussion that follows you will be encouraged to reflect on the philosophies of family- and child-centred care, what they mean to you in your practice, the points of tension and challenges that exist, and the care of children, young people and their families more generally. The case study provides a means for reflection on how children and families experience health care and what informs ways of working with them. This includes some of the taken-for-granted aspects of care and also best practice and possibilities for achieving child- and family-centred care.
A number of assumptions underpin the discussion throughout the chapter. Firstly, children and young people experience illness, injury and disability in a different way from adults and their health care needs are therefore quite different to those of adults. Further, children’s and young people’s developmental immaturity leads to certain vulnerabilities. Their vulnerability is not an inherent consequence of childhood or adolescence as such, but a result of adult-centric social structures and services that children and young people cannot access as easily as adults. In addition, childhood and adolescence are characterised by rapid physical, cognitive, developmental, social and experiential changes. Children’s and young people’s dependence on adults is naturally on a continuum of dependence to growing independence – although this latter point may not necessarily be the case for children with long-term complex conditions (Children’s Hospitals Australasia 2010). Care of children and young people also involves unique considerations in terms of communication, consent (or assent) and confidentiality (Ford et al. 2007).
Societal and economic impacts provide varying contexts for children’s lives in the 21st century. For example, women’s increased participation in the workforce and changes to family structures (including the increased numbers of single parent families and of childless families) impact on children within families and in the broader society. Intergenerational relationships also need consideration, particularly with the increasing numbers of frail older people requiring care and support within families and society (Christensen and Prout 2005: 51).
Children and young people experience health care services in many different settings, such as in their homes, their community and in hospital settings. While much of the literature relates to the care of children in hospital, it must be acknowledged that health care for children largely takes place outside of hospital wards and clinics. Caring for children with complex needs within the home, for example, poses different and sometimes quite complex issues about how health care professionals work in family-centred ways (Kuo et al. 2012).
A further important assumption for nursing children and young people is that nurses who provide this care need to have well-developed skills to recognise the particular health, psychological, emotional, developmental, communication and cultural needs of each child and young person (Hill et al. 2011: 80).
An historical context of children’s health care
Tracing the historical place in which children and young people have been positioned in health care, whether that care is within the community or in hospital, shows that it has been largely influenced by their positioning within society more generally. The roles families play in their child’s health care have also been impacted by social drivers. Advances in preventative health such as the impact of immunisation as well as treatments and technology, policies and legislation (most notably of course in affluent societies) have also shaped how and where children and young people are cared for. Once fatal childhood diseases such as congenital heart defects or leukaemia are now treatable, and many children in countries with appropriate resources can now survive into adulthood (Stang and Joshi 2006).
When considering the history of the care of children in hospital, the 19th and earlier part of the 20th centuries saw parents excluded from the wards and denied the opportunity to be with their child. The understanding at that time was that children in hospital settled better when parents did not visit. During this same period, parents of children with severe disabilities were strongly urged to institutionalise their children, resulting in these ‘hopeless cases’ being physically removed and separated from their families. The environment considered suitable for the hospital-based care of children has changed considerably since the first wards built for children. Figure 1.1 shows a photograph of a children’s ward at the beginning of the 20th century and Figure 1.2 shows architectural drawings of the wards of the ‘Hospital in the Park’ in Liverpool, UK, which is due to be completed in autumn 2015. These starkly contrasting environments reflect very different ways of thinking about what is necessary to be able to deliver good health care to children.
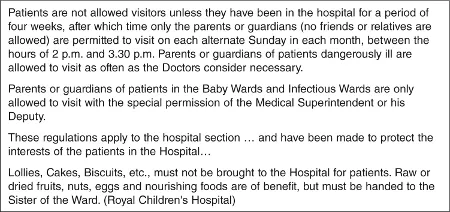
The hospital rules from a children’s hospital in 1947 limiting parents visiting their hospitalised children are presented in Figure 1.3. The strict and inflexible rules outlined here appear similar to those for visiting prison inmates (Street 1992). While the regulations and practices intended to safeguard the best interests of the ill child, such practices did not support the interests of the parent or child so much as institutional interests (Street 1992). For example, medical staff determined how often, and for how long, children might be with their parents.
The strong emotional reactions of children to their parents when they were allowed to visit was seen as evidence that parental visits had a detrimental effect on children’s well-being. The recognition that the practice of separating children and parents could cause possible psychological trauma to children who experienced hospitalisation was slow to develop. Following on from societal reactions to the effects World War II had on the separation of children from their families, the subsequent work of people such as child psychologists John Bowlby and James and Joyce Robertson on separation, and reports such as the Platt Report (Ministry of Health 1959), children’s health care in the second half of the 20th century saw changes in care practices. As a result, the involvement of parents in the care of their sick child became an accepted feature of children’s nursing. In Australia, daily visiting for children was adopted in the 1950s and 1960s and mothers whose young babies were sick were able to be with their children in hospital in the late 1970s (Wood 2008: 123). Sibling visits and parents accompanying their children to theatre were other changes to care practices around this time (Kuo et al. 2012). However, the recognition that the interests of children, young people and families should be at the centre of children’s health care was slow to pervade all areas of children’s health care.
The description by Joy Chester – founder of AWCH (the (Australian) Association for the Wellbeing of Children in Healthcare), of her experiences around the admission to hospital of her child illustrates this:
The current context of children’s health care
Despite significant progress and initiatives to address the negative experiences of children who are hospitalised, children continue to experience physical harm, unnecessary pain, fear and anxiety during and after health care experiences (Nicholson and Clarke 2007). A number of reports and inquiries have highlighted continuing deficits in health care services where bureaucratic and systemic interests have been privileged over those of children and young people. In the UK, for example, the Bristol Inquiry Report was instigated in response to the deaths of some 30 to 35 children undergoing cardiac surgery between 1991 and 1995 that were found to be the result of major ‘flaws and failures within the hospital, its organisation and culture’ (Kennedy 2001: 154). The report found that in health care services children were treated as ‘mini adults’, simply needing ‘smaller beds and smaller portions of food’ and that information was not provided in a suitable form for children or their parents. Further, it was reported that staff did not have specific education in caring for children and that the facilities did not meet the special needs of young children, older children, adolescents or parents (Kennedy 2001: 12). The Garling Report (2008) was conducted in the Australian state of New South Wales and included a review of health care services for children and young people following adverse events that shocked the public, including the death of a young person whose care was found to be inadequate. These reports and others have led to significant policy and practice changes that emphasise the importance of placing children, young people and families at the centre of care. Many policies that have been developed for the standards and rights of children’s and young people’s health care are framed by the United Nations Convention on the Rights of the Child (UN 1989) that encapsulates the universal rights of children.
The UN Convention on the Rights of the Child (UNCRC) was adopted by the United Nations General Assembly in 1989. It acknowledges the status, role and rights of children and their needs and situations by setting standards in health care, education and legal and social services (UN 1989). Articles of the Convention that directly relate to health care are outlined in ...