![]()
1
Administrative Capacity
and Health Care in Africa
Path Dependence as a Contextual Variable
CAMERON WIMPY, MARLETTE JACKSON,
AND KENNETH J. MEIER
Management clearly matters in a wide variety of both national and substantive contexts—ranging from public schools in the United States, the Netherlands, and Denmark to local governments in England and Colombia to national governments. The impact of management on different aspects of performance, however, varies across these different contexts. In the introduction to this book, O’Toole and Meier present a theory of context whereby context is expected to interact with management and condition the results of public management on performance. Ideally, they argue that one would study management across contexts so that context might be a variable that could be used as an interaction effect within a single equation (see equation 2 in the introduction). Their second-best proposal is for scholars to document the context of their studies along such dimensions as the political context (the degree to which political power is concentrated), the environmental context (complexity, turbulence, munificence, and social capital), and the internal organizational context (goals, centralization, and professionalism). We follow the first strategy in this chapter by examining the role of administrative capacity in health outcomes in thirty-six African countries, using the path dependence of being a British colony as the contextual variable.
The analysis proceeds in five parts. First, we introduce the concept of administrative capacity—a variable that is often assumed in studies of public management but rarely measured and included as an explanatory variable. Second, we present a theoretical argument that bureaucracy or administrative capacity is subject to path dependence. The creation of administrative capacity takes time to develop, and the effectiveness of administrative capacity should be enhanced to the degree that bureaucracy has a longer history of effective performance. We use experience as a former British colony as our indicator of effective historical performance, based on a reading of the qualitative historical and political literature. Third, we introduce the substantive area of concern, health outcomes in Africa, with a focus on a health care indicator, child mortality, that should be highly sensitive to administrative capacity and the ability to deliver basic services. Fourth, we present a panel analysis of thirty-six African countries over an eleven-year period that shows administrative capacity is associated with significant reductions in child mortality and that these reductions are significantly greater in former British colonies. Additional analysis examines the same relationships for the incidence of cholera, HIV infections, malaria, and tuberculosis (TB) and also suggests that the effects are nonlinear. Fifth and finally, we assess the meaning of the present analysis for the study of how context conditions the impact of management on performance.
ADMINISTRATIVE CAPACITY
Administrative capacity or, alternatively, the quality of administration is a central feature of governance. Policies are rarely self-implementing, which dictates the establishment of an administrative organization to oversee programs and deliver actual services. In most cases, policy actions are expressed as goals—the improvement of health outcomes, the reduction in poverty, the increase in human capital, creating democratic citizens—and the specific programs are left for administrative agencies to design and implement (Rourke 1984). This aspirations form of policy in turn requires a level of administrative expertise to understand the causal linkages in the policy under question, or in some cases to discover such linkages and design solutions. Administrative capacity is needed for this, and government bureaucracies are the political institution that is most designed to develop policy expertise. All bureaucracies engage in specialization and breaking down complex problems into smaller parts where the solutions might not be as daunting. The logic of near-decomposable systems (Simon 1965) holds that these small solutions can then be reaggregated in such a manner as to generate an effective overall policy. Bureaucratic specialization is facilitated by the hiring of professionals and technicians with specific skills that are applicable to the problem being addressed. Administrative capacity in this manner should be directly associated with administrative quality because it permits the organization to make better decisions.
Administrative capacity is also linked so closely to two other concepts that they may be descriptions of the same phenomena. Administrative stability as a concept taps into a bureaucracy’s permanence and its ability to address problems by breaking them down over time or by using prior experience to solve problems. Although one might use turnover or some other indicator of administrative stability, it is often measured as the size of the administrative component (see chapter 4 in this volume, by Torenvlied and Akkerman). Similarly, there is a literature examining the concept administrative intensity, an organization’s relative ratio of administrative effort to production, as a dependent variable (Boyne and Meier 2013). This literature is driven by two predominant hypotheses—the public choice hypothesis, that administrative intensity is a function of bureaucratic waste and aggrandizement; and the functional hypothesis, that administrative intensity is an effort to address organizational problems. In the later interpretation, administrative intensity can be considered the equivalent of administrative capacity, with its links to improved organizational outcomes.
Despite this universal understanding of administrative capacity and its linkage to administrative quality and role in effective programs, the public management literature has generally ignored capacity. Many studies examine a set of organizations that are well established, and among which the range of administrative capacity is relatively small and thus becomes treated as a constant in the process. Even within such studies, variation in capacity is often difficult to measure and is often indicated by very indirect indicators, such as the size of administrative staff (Bowman and Woods 2007; Huber and McCarty 2004; Johnson and Randall 2013; Meier, O’Toole, and Hicklin 2010).
Indirect measures such as size have one inherent limitation. Bureaucracies can be large because they are specializing and developing expertise, or they can be large because they are inefficient but have still convinced the political branches to fund them. Better measures of capacity actually try to assess quality—the ability of the bureaucracy to effectively implement policy. In most cases such measures are based on elite opinion, using a set of raters that have experience with the governments in question. Within the United States, perhaps the foremost example of elite measures of administrative capacity is the Government Performance Project (Ingraham, Joyce, and Donahue 2003; Ingraham 2007; for an application, see Krueger and Walker 2010). A parallel measure for many developing countries, including those in this study, has been created by the World Bank (see below).
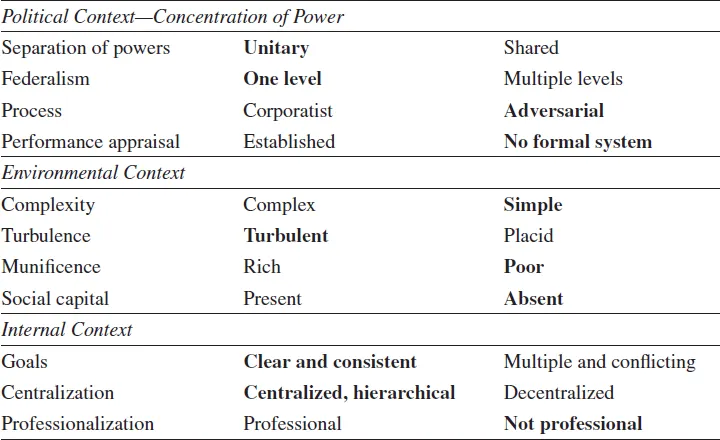
The objective of this chapter is to relate administrative capacity to health outcomes in Africa (see table 1.1 and the discussion in the conclusion for a more detailed description of how this setting fits into the context matrix). The impact of administrative capacity or public administration quality on health care outcomes is relatively straightforward. The greatest relative gains in health outcomes tend to be preventive measures that protect individuals from diseases that could lead to premature death. Health care in these situations is not the high-technology type of care associated with major medical centers but rather primary care, immunizations, sanitation, and other relatively simple actions. In the countries under study, this involves dealing with malaria, TB, cholera, and HIV infection, as well as providing prenatal care and primary care health workers. The ability of government bureaucracies to carry out such programs, particularly to implement them outside the capital city, becomes essential. Administrative capacity should be a good measure of the ability to effectively implement these large but low-technology health care programs. The impact of such programs should be felt most on overall indicators of public health, such as child and infant mortality rates (Gupta and Verhoeven 2001). The influence of administrative capacity in Africa generally takes place in a political context characterized by unitary nonfederal system governments with adversarial processes and no formal performance appraisal. Environments are complex and turbulent but poor and lacking in social capital. The internal context is centralized but also nonprofessional and associated with multiple and conflicting goals. These generally problematic contexts for policy places a high premium on administrative capacity.
Table 1.1 The Public Management Context Matrix: African Countries and Primary Health Care
PATH DEPENDENCE
The impact of administrative capacity on government program performance is quite likely to be affected by context. Bureaucratic capacity can easily be undercut by a lack of resources, by a corrupt political system, or by a variety of other factors. This study will take one of these contextual factors—path dependence—and illustrate how it conditions the impact of government capacity. Government bureaucracies deal with problems by breaking them into small parts and fixing one part at a time. When such policies rely on the cooperation of citizens, the bureaucracies need to repeat the process as new clientele arrive until the resulting behaviors or conditions change. Health care is particularly affected by this long time frame and path dependence. Immunization programs, prenatal care, clean water, sanitary systems, and similar preventive efforts require continued operation to do intake for new clientele, to maintain water systems, to distribute nutritional information and supplies to expectant mothers, and the like. Health is a coproduced good, so it requires high levels of trust among the population, which can take time to develop.
Our measure of path dependence is a simple one that codes whether a country is a former British colony. Although all colonial governments in Africa were exploitive and focused on generating returns for the home country rather than developing effective future governing structures, scholars generally perceive the British experience as least abusive (Agbor 2011; Barro 1999; Clague, Gleason, and Knack 2001; Lipset, Seong, and Torres 1993). The expressed philosophy of British governance was indirect rule, whereby indigenous rulers were co-opted by the British to assist in governing (Herbst 2000, 81).1 This symbiotic relationship meant that British colonies had a vested interest in developing local bureaucratic capacity by investing in education for local administrators and training in administration and management to a greater degree than in other African colonies (see Kingsley 1967, 307). This investment meant that at the time of independence, the British colonies in Africa had, on average, greater indigenous administrative capacity than did the French, Portuguese, or Belgian colonies. This legacy also meant that former British colonies had a head start in distinguishing between the administrative state and personal gain, so that increases in administrative capacity were built on a stronger base than in other colonies. The generalist nature of the British administrative service meant that after independence, the former colonies could enter into contracts with foreign officials for their technical and scientific expertise and at the same time retain key management positions in the bureaucracy (Kingsley 1967, 309).
The experience of the former British colonies differs markedly from other forms of colonial heritage. For example, when the Portuguese left Mozambique in 1975, there were no trained Mozambican doctors (Walt and Cliff 1986).2 By contrast, Grier (1999) concludes that many of the existing differences in postcolonial development between the British and French colonies can be explained by education levels at the time of independence. In the case of the French colonies, the existing power structures were often reorganized and major responsibilities of governance were most often carried out by French officials. Conversely, the British colonies experienced far less meddling in existing local power structures when compared with the French (Crowder 1964). In a study of the Hausa peoples, who inhabit the overlapping Hausaland region of Nigeria and Niger, Miles (1994) concluded that there were marked differences in development in Nigeria (a former British colony) when compared with Niger (a former French colony). These findings were further echoed in a more recent case study of Cameroon (Lee and Schultz 2011), which was split into two colonial administrations (British and French).3 The authors concluded that the British-administered area of West Cameroon had higher levels of public goods provisions and better-performing local governance institutions when compared with the French-administere...