![]()
Part One
Bipolar Disorder in Children
Dealing with sudden rage, aggressive depression,
oppositionality, and crazy thinking
![]()
CHAPTER 1
Enter the Warrior
How to Identify the Presence of Bipolar Disorder in Children
‘The profile of the child at risk for bipolar illness suggests that whatever emotion – negative or positive – these children experience, they seem to experience it intensely or passionately. Their behavior is likewise dysregulated and disinhibited.’
Dr Hagop Akiskal
The archetype: The Warrior
The child with Bipolar Disorder occupies the Warrior archetype and possesses the gifts and challenges of that temperament. He is a risk taker. He is the opposite of a ‘cool character,’ and has a ‘hot ’ personality which relishes the clean decision of combat. He makes quick judgments. He wants to know what’s in it for him. If you cross him or disagree with him, he will challenge you and will attempt to dominate you.
THE GIFTS
The Warrior thrives on intensity. He will create a fight just to make things interesting. He has the wisdom gained from experiencing the highs and lows of existence. He may have gifts in literary and creative artistry. He has a powerful will to achieve his goals and does well in academic areas. He is fierce as an enemy.
THE CHALLENGES
He can be his own worst enemy. The excess of fire in the temperament of the Warrior is his biggest challenge. He can become powerfully isolated from others because of his rage and impulsivity which may flare out of nowhere. His self-centeredness and hunger for stimulation and excitement can make him a monster in the eyes of others. In his moments of depression, he may decide to take his own life or undertake other forms of self-destruction to escape the depression.
Jessie: Profile of a child living the Warrior archetype
She is seventeen. Her name is Jessie. At four, she showed signs of being obsessional about things. She could not sleep unless her toys were lined up just so. She always had to even up everything. She had night terrors – vivid half-awake, half-asleep nightmares as if she were on a bad acid trip that defied attempts by her parents to wake her up. The worst of it were her rages which began around age five. They would emerge like sudden, violent windstorms at the least frustration and could go on for an hour or more. Enraged she spit, hit, frothed at the mouth, laughed, cried, attacked her parents, tore up her prized teddy bear and toys. Enraged, she was a little wild creature. Her parents had to hide sharp objects as she would take them and gouge their things or attempt to throw heavy objects at windows or the TV screen. She complained that she could not get voices out of her head that told her to do destructive things.
Despite these disturbances, Jessie held it together at school and was fiercely determined to get good grades. She excelled in literature and writing and was very creative. But after school she could get crazy. The rages would come at this time along with the suicide threats and the attacks on her parents. A couple of times, at age nine, she had grabbed the steering wheel of her parents’ car and tried to turn the car into oncoming traffic. She was extremely impulsive. Nothing her parents did stopped her from doing exactly what she wanted at any particular time. She tried to light the house on fire. She went after Jester, her family ’s beloved Toy Collie, with a knife and would have killed the dog if her father hadn’t been there to wrestle the weapon away from her. She showed little remorse for her actions and seemed to be entirely self-centered.
Hitting puberty, she became more obsessional and more aggressive. Her parents felt relief when she was out of the house. When she was home, she would stalk them for hours, swearing at them and taunting them. She appeared to crave their angry response and would come out of the blue with an insult in an attempt to start a fight. At age fourteen, she fell into a depressive funk. She could not get out of bed in the morning. Nothing interested her. Her parents were taking it one day at a time – trying to get through to their miserable, brilliant, totally self-centered daughter.
At fifteen, her parents sent her to a residential school in Utah that had other boys and girls with her problems. The therapeutic milieu, structure of the place and the absence of opportunities for her to hurt herself worked to help her stabilize her life. It was there that her psychiatrist was able to find the right mix of medication to help her after diagnosing her with early-onset Bipolar Disorder. Her doctor prescribed one of the newer anticonvulsant medications along with lithium and her mood stabilized greatly. The addition of an antidepressant medication brought her out of the funk she had been in for years. At the time of this writing, Jessie is finally acknowledging the presence of Bipolar Disorder in her personality. There is a good possibility that she will be able to attend college in a couple of years. Things are beginning to look up.
Physicians are beginning to accept the fact that children like Jessie may be suffering from a disorder that, up until a few years ago, was thought not to occur in children her age. She shows a pattern of behavior that she shares with many adults now diagnosed with Bipolar Disorder.
What Bipolar Disorder in adults looks like
The Diagnostic and Statistical Manual IV (DSM-IV), the diagnostic guide used by psychiatrists, defines Bipolar Disorder by the presence of manic or hypomanic states and depressive states, which alternate in various patterns.
Hypomania and mania
Hypomania is a term which describes a mild form of the inappropriately elevated mood of mania. In hypomania the person’s mood is overenergized – ‘elevated, expansive, or irritable,’ to use the DSM-IV language – but the person is not disabled by this mood ‘high’ and does not suffer from ‘marked impairment in function.’ In fact, many persons with Bipolar Disorder report that they value the hypomanic phase, as it is a time when they are most productive, as if they are running on ‘high test’ gasoline and enjoying the feeling.
One person who experiences hypomania describes the experience (from a pamphlet published by the National Institute of Mental Health):
At first when I’m high, it’s tremendous. Ideas are fast, like shooting stars you follow until brighter ones appear. All shyness disappears, the right words and gestures are suddenly there. Uninteresting people, things become intensely interesting. Sensuality is pervasive, the desire to seduce and be seduced is irresistible. Your marrow is infused with unbelievable feelings of ease, power, well-being, omnipotence, euphoria. You can do anything. But, somewhere this changes.
For some people the change is to a manic state. In the DSM-IV, a manic episode is defined as ‘a period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary)’ and ‘in which the mood disturbance is severe enough to cause marked impairment in functioning.’ Other characteristics include talkativeness, mind-racing, distractibility, wild pursuit of goals, and excessive concern with ‘pleasurable activities that have a high potential for painful consequences’ – sexual indiscretion, gambling, etc.
The fast ideas come too fast and there are far too many. Overwhelming confusion replaces clarity. You stop keeping up with it – memory goes. Infectious humor ceases to amuse. Your friends become frightened. Everything is now against the grain. You are irritable, angry, frightened, uncontrollable, and trapped.
Depression
Dr Michael Norden, a Seattle-based expert on Seasonal Affective Disorder, a form of depression, uses the acronym ‘APES SWIM’ to define the key somatic/psychological characteristics of depression (Norden 1995, p.7). When these symptoms are severe, the person is said to be suffering from ‘major depression.’
Somatic symptoms
A:appetite or weight reduction or increase (5% in a month)
P:psychomotor retardation or agitation (moves slowly, or is jittery)
E:energy reduction (fatigue)
S:sleep reduction or increase
Psychological symptoms
S:suicidal ideas or thoughts of death
W:feelings of worthlessness or inappropriate guilt
I:interest or pleasure decreased in most activities
M:mental ability, concentration, focus, decision-making, decreases
The depressed state is described well by another Bipolar patient:
I doubt completely my ability to do anything well. It seems as though my mind has slowed down and burned out to the point of being virtually useless. I am haunted with the desperate hopelessness of it all. Others say ‘It’s only temporary, it will pass, you will get over it,’ but of course they haven’t any idea of how I feel, although they are certain they do. If I can’t feel, move, think, or care, then what on earth is the point?
The six variations of Bipolar Disorder
The DSM-IV describes two different variations of Bipolar Disorder. These two types differ in that they define different combinations of mood strength and frequency of mood shift.
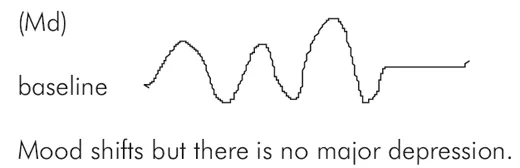
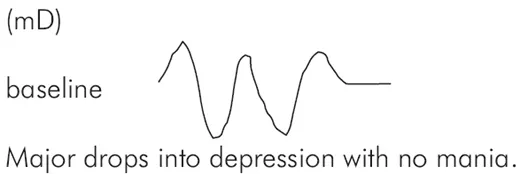
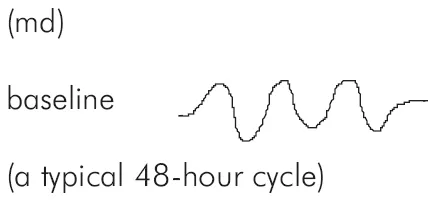
(In the graph parentheses seen below, ‘M’ stands for ‘mania’ or ‘hypomania’ and the ‘D’ represents ‘depression.’ A small ‘d’ or ‘m’ represents a mild or insignificant amount of the mood type. The strength of mania and depression is graphed from a baseline of ‘normal’ or ‘stabilized’ mood.)
Bipolar I Disorder is described as the presence of a single episode or several episodes of mania, hypomania or depression with no incidence of major depression. Bipolar I might be described like this:
Figure 1.1
Bipolar II Disorder is described as the presence of recurrent major depressive episodes with hypomanic interludes in between the dives into depression. In order to meet the criteria for Bipolar II, there can never have been a manic episode in the person’s history.
Figure 1.2
Four other types of Bipolar Disorder have been identified.
Though the DSM-IV does not yet list varieties of Bipolar other than the types listed above, psychiatrists and other practitioners refer to four additional types drawn from the work of Young and Klerman (1992). Again, frequency of mood shift and the character of that shift define these types:
Bipolar III – Cyclothymic Disorder – manifests as cycling over short intervals between hypomania and mild depression. Cyclothymia is not diagnosed if there is evidence of major depression. In Cyclothymia highs are less high, and lows are less low than in the Bipolar I or II varieties.
Figure 1.3
Cyclothymia may be expressed in rapid cycling on a daily basis, beginning with a depressive phase in the morning and leading into a manic phase in the late afternoon and evening.
Bipolar IV – antidepressant-induced hypomania – is not yet listed in the DSM-IV but will probably be in the next edition of the manual. This diagnosis defines a condition in which hypomania is induced by the administration of antidepressant medications such as fluoxotine (b. Prozac) or fluvoxomine (b. Luvox), and the tricyc...