![]()
1
Stress factors
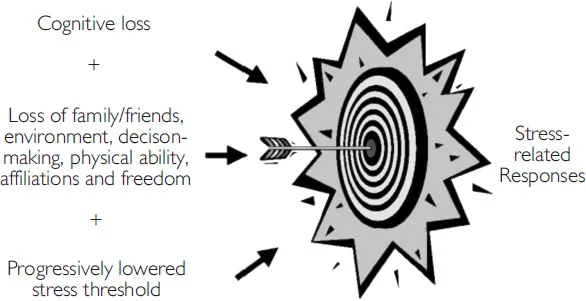
The development of dementia causes cognitive loss (loss of mental processes of comprehension, judgement, memory and reasoning) and conative loss (involving changes in behaviour and actions) in many cases perceived as personality changes. Stress-related behaviours, often referred to as Behavioural and Psychological Symptoms of Dementia (BPSD), commonly emerge as the condition progresses and, besides being a burden to the sufferer, can be distressing for carers (Hart et al. 2003). These behaviours may be the result of a progressively lowered threshold to stress (Hall 1994) or ‘shrinking of the comfort zone’ (Caron and Goetz 1998) resulting in stress-related responses such as agitation and aggression. Triggers such as loss of family and friends, a comprehensible environment, decision-making responsibility, physical ability, affiliations and freedom increase susceptibility to these stress-related behaviours.
Short-term memory is usually lost first, while long-term memory is retained. Thus people with dementia may find present places, faces and practices unfamiliar and stressful. They may feel as if they are surrrounded by strangers.
Pre-existing pathological conditions, personalities or character styles, or neurochemical or structural abnormalities in the brain, may underlie stress-related responses in people with dementia (Dyck 1997). Depression is more common in people with dementia than in non-demented people and this may result in their being more emotionally vulnerable to stress (Verhey and Visser 2000). These factors in association with cognitive impairment reduce tolerance to adverse environmental stimuli (such as unfamiliar routines, care practices or environments) (Raskind 1999).
Common stressors that may overwhelm a person’s reduced coping threshold include:
•mental and physical fatigue
•change of daily routine, caregiver or surroundings
•misleading stimuli or inappropriate stimulus levels
•excessive internal or external demands to achieve beyond their functional capacity
•physical stressors such as pain or physical irritation, infection, dehydration or depression
•affective response to perceived functional losses of day-to-day skills and independence
•loss of ability to communicate needs and comprehend spoken words.
(Hall 1994; Hall and Buckwater 1991)
People with dementia can be frightened or anxious when exposed to stressors. Their capacity to cope can be easily exceeded in a situation of failure (Hall, Kirschling and Todd 1986).
The losses associated with dementia may be further compounded by ‘excess disabilities’: the presentation of reversible symptoms of functional incapacity greater than warranted by physiological impairments. Excess disability may result from unrecognized or inadequately treated medical conditions, medications, or various emotional, psychological and environmental factors. Medical burden is of course a source of excess disability but sensory loss due to unsuitable spectacles or wax impaction of the ears can lead to decreased cognition, hallucinations, delusions, emotional lability, isolation and agitation (Morley and Miller 1993). Medication side-effects can produce unnecessary disability, and care techniques that assist the person to perform tasks which they would still be capable of performing for themselves (albeit slowly) can lead to excess dependency for activities of daily living. Environmental complexity resulting in difficulty accessing the toilet can promote unnecessary incontinence. Muscles that are not used may deteriorate.
Imagine your reactions to the following situations:
You are driving the family to see your spouse’s parents. You have other things you would prefer to do. In fact the only time a trip to visit the parents-in-law in Italy could be arranged happened to be the week of the annual fishing trip, which you haven’t missed for ten years. You are jet-lagged, have a headache, can’t stand driving a Fiat, it’s turned dark and you cannot see or read the road signs. In fact you are lost, and the kids are conducting a war in the back seat. Still you are keeping your cool…just. Then your adorable teenage daughter indulges in a truce with her brothers for long enough to say, ‘I bet you forgot to bring the present for grandma.’ That was an odds-on bet, so you now add a feeling of disrespect and failure to your stress and frustration.
You would probably cope better with this situation:
You have had a good day. You are celebrating a success by buying yourself that special perfume. As you stand at the counter savouring the moment, a passer-by gives you a little push or bump to get through a congested aisle. You probably cope with this well.
Now let’s look at the same event under different circumstances:
You have had a really bad day; you lost your job, the pet dog is missing and you have dented your car. You are buying a gift that you can ill afford for an aunt you don’t particularly like but are obliged to honour appropriately.
How do you feel now when pushed by the impatient person? Is your stress threshold or tolerance reduced?
Results of stress
Naturally stress will result in overall poor health outcomes, agitation, a reduced ability to attend to activities of daily living, and will make care more difficult and less pleasant.
Billing (1996) indicates that stress can also lead to:
•physically aggressive behaviour such as hitting, scratching, spitting or biting
•verbally aggressive behaviour such as abuse or cursing
•physically non-aggressive behaviour such as inappropriate disrobing, wandering or intrusiveness
•verbally non-aggressive behaviour such as yelling, incessant demands or constantly repeating words or remarks.
A person with dementia may live with frustrations, losses and reduced tolerances, and consistently be adversely affected by seemingly minor or imagined insults or stresses. That can be the world of the person with dementia. People with dementia need care that finds and accounts for what they want to do, cures the headache, minimizes disruption, simplifies life for them, avoids fatigue, interprets the environment, respects them and doesn’t challenge them or ask silly questions.
Feeding and sleeping problems, although not necessarily stress-related, may also be evident in people with dementia, and be a challenge to manage.
![]()
2
Preventing/minimizing stress
Providing the best care for people with dementia exhibiting stress begins with a thorough assessment to search for underlying causes of behaviour change. Concomitant medical illness should be treated and sensory impairment addressed. Assessment and management are essential components of the treatment of dementia (Herrmann 2001).
Find out as much as you can about the person
As long-term memory is preserved longer than short-term memory in dementia, the world as seen in the mind of the person with dementia will often be in the distant past. Thus care practices need to be based on an intimate knowledge of the person’s life. We also need an accurate picture of how the person is functioning at significant points in time, such as on admission to residential care. Establishing a baseline is also important so that we can objectively validate the outcomes of care practices.
Establish a baseline of function
On admission to residential care, it is important to assess cognition, mood, performance of activities of daily living, mobility and general function. For people being cared for at home, a community nurse or a doctor, possibly by referral, could gain this information.
•Conduct baseline tests of cognitive status such as the Mini-Mental State Exam (MMSE) (Folstein, Folstein and McHugh 1975), which provides a score out of 30 to assess memory, orientation (knowledge of time and place), comprehension, attention (ability to maintain focus), command of language visuospatial skills (ability to process and interpret visual information about where objects are in space) and motor skills.
•Assess mood. Various geriatric depression scales are available and may be suitable for some patients. However, depression may fluctuate, the patient may be ‘stoic’ or answers may be affected by cognitive loss and result in responses that underestimate the likelihood of depression. If this is suspected to be the case, gain information from someone close to the person (Rubin et al. 2001) and document mood in the interview and in the performance of the mental states examination. Depression in elderly individuals is associated with reduced cognitive test performance, especially in more complex and time-demanding tests and tests of memory (Palsson et al. 2000).
•Document general presentation, level of awareness, attitude to the interviewer, ability to understand and communicate information and whether thought processes are logical. Besides word-finding abilities, people with dementia may also have an impaired ability to receive information logically.
•Check if the person has insight into their disability. Those who have insight may be more prone to depression, whereas those without may be more prone to paranoid ideation.
...