![]()
— PART I —
FOCUSING
THE GAZE
![]()
— Chapter 1 —
SETTING THE SCENE
Introducing Portraiture as a ‘Third Hand’ Intervention
I wanted to begin this book with a story that succinctly described how portrait therapy grew out of the issues presented by the patients I worked with over many years in palliative care, something thoughtful and profound, or at least something that showed my insight and sensitivity to these issues. Yet as I sit here at the computer my mind refuses to give forth its profound thoughts, and instead reminds me of my awkward and embarrassing moments. My first experience of working in palliative care was as an art therapy student over 12 years ago, it was during the second week of my placement and I was sat around a table with five patients, their faces all looking at me expectantly. ‘What are we going to do today then?’ asked one lady. ‘I can’t draw a straight line!’ joked another. ‘Well,’ I said nervously, ‘today I think we shall begin by painting a picture of how our week has been…’ As I spoke I was filling some pallets with some very liquid poster paint, newly bought for the group, but the yellow paint was proving particularly stubborn and refused to flow from the narrow plastic spout in the lid.
In hindsight just squeezing harder on the belly of the bottle was obviously a mistake, because at that moment the whole lid decided to fly off and the contents of this lurid yellow paint flew in all directions, splattering these severely ill patients from head to foot in yellow spots. After a second or two of stunned silence hilarious laughter broke forth, as the patients turned around and looked at each other, tears of laughter running down their cheeks mingling with the yellow paint. Needless to say, this story went around the hospice causing much hilarity; however, later that day I overheard one elderly lady say that the art therapy group was ‘the best medicine’ she’d had all week and that she ‘couldn’t wait to get home and tell her husband all about the yellow paint!’ This was, I guess, my first experience of ‘painting’ my patients…
Despite my inauspicious start, at the end of my training I was offered a position as an art therapist at this same hospice, and my journey towards the development of portrait therapy began. My art therapy practice is based on the ‘studio art therapy’ model outlined by Catherine Moon (2002), and other art therapists concerned with keeping the focus on ‘art’ within art therapy (Allen 1992, 2001a, 2001b; Brown 2008b; Cahn 2000; Malchiodi 1999a; McNiff 1986; Robbins 2000; Wix 2000). This model aims to avoid the ‘clinification’ of art therapy (Allen 1992, p.23), something that art therapist and writer Pat Allen says ‘neglects to employ the very specialized knowledge that derives from our background in art making itself’. Allen’s (1992) open studio model works on the premise that it is part of the art therapist’s role to pursue his or her own art making as a way to create ‘a bridge to and from her core self to her role as therapist’ (ibid., p.26). And as Reason (2006, p.188) says:
If we start from the idea that creating knowledge is a practical affair, we will start not, as in traditional academic research, from an interesting theoretical question, but from what concerns us in practice, from the presenting issues in our lives.
Within portrait therapy, I acknowledge that my therapist and artist identities merge, and as an art(ist)-therapist I believe in the power of art to heal, challenge, and transform meaning (Adamson 1984; Stuckley and Nobel 2010), and to build bridges between our discursive and non-discursive selves (O’Brien 2004). The creation of art has played an important role in all known cultures around the world (Dissanayake 1988) and there is extensive anecdotal and growing empirical evidence that art therapy and the arts have a contribution to make in the health and well-being of those living with life-threatening and chronic illnesses (Connell 1992, 1998; Hill 1945, 1951; Kramer 1971, 2004; Luzzatto 1998; Malchiodi 1999b, 2007; McNiff 1992, 2004; Pratt and Wood 1998; Waller and Sibbett 2005).
Portrait therapy is grounded within the ‘holistic’ paradigm, with its focus on the physical, emotional, psychosocial and spiritual aspects of a person’s experience of illness (Saunders 1976, 1990). Central to the ethos of palliative care is the improvement of patients’/clients’ ‘quality of life’ (Bell 2008, p.354), and this, along with the empowerment of individuals, is the overarching aim of portrait therapy. As Judith Herman says (1992, p.133), ‘The first principle of recovery is the empowerment of the survivor. She must be the author of her own recovery. Others may offer advice, support, assistance, affection and care, but not cure.’
Within portrait therapy an attempt is made to equalise the relationship between art therapist and patients through the develop-ment of a collaborative intersubjective relationship. Within this relationship the patients, in a series of negotiations, co-design their own portraits directing how they wish to be portrayed. The co-designing process and viewing of the portraits provide a unique way of looking at the phenomena of disrupted self-identity and embodiment, enabling patients to see themselves through the eyes of an empathic and attuning ‘other’. This, therefore, is the foundation for the collaborative and intersubjective relationship: ‘Paint me this way!’
What is self-identity disruption?
My interest in using portraiture as an intervention developed from a growing recognition and concern for the disruption to self-identity caused by life-threatening and chronic illnesses that many of my patients talked about on a daily basis. Self-identity disruption is characterised by statements such as ‘I don’t know who I am any more’, or ‘I’m not the person I used to be’, and ‘I look in the mirror and I say “who’s that?”’ Indeed, patients often describe the impact of their diagnosis, treatment and illness as having changed their sense of self-identity beyond all recognition (Charmaz 1983).
Very early in this research process I discovered this quote describing identity disruption, by counselling researcher Mitchell B. Young (1988, p.32). He said:
To have one’s identity disrupted is to travel without a compass…
This captures the essence of self-identity disruption, describing succinctly a sense of displacement, disorientation and disempowerment, of not knowing which way to turn, or who they are now they are ill (Corbin and Strauss 1987). This sense of disorientation clearly causes problems in all aspects of a person’s life/world, impacting on decision-making, relationships with significant others and most importantly their relationship with themselves. As Bolen (1996, p.14) says:
Illness is both soul-shaking and soul-evoking for the patient and for all others for whom the patient matters. We lose an innocence, we know vulnerability, we are no longer who we were before this event, and we will never be the same.
The diagnosis of a life-threatening illness and the steady deterioration of a chronic illness also negatively impacts upon a person’s ‘creative capacity’ to adapt to illness (Reeve et al. 2010), and their quality of life (Carel 2011; Crewe 1980; Mathieson and Stam 1995; Toombs 1988). It can cause: increased stress, loss and grief; loss of meaning and disruption to future goals (Falvo 1999), and commonly results in depression and social isolation (Rodin et al. 1991). Research has demonstrated that aside from all the other stresses faced by those living with life-threatening and chronic illnesses, social isolation on its own can reduce immune function, cause depression and shorten life expectancy (Jaremka et al. 2012), suggesting the importance of developing effective interventions such as portrait therapy, where the relational aspects of self-identity can be validated.
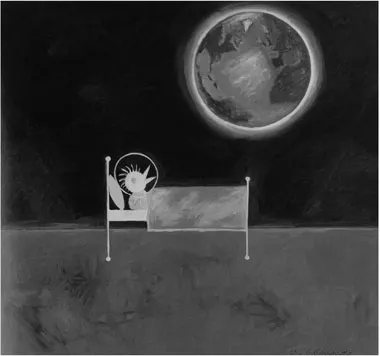
Figure 1.1 Out of This World by John D. Edwards © 1999 (see also Coloured Plate vi).
In this painting called Out of This World (Figure 1.1) artist John D. Edwards (2007) conveys his experience of social isolation and disruption to his life and self-identity caused by his experience of cancer. Edwards’ experience is echoed by Claire Smith (2008), talking about her own experience of ‘deep illness’ (Frank 1997):
I live in a bubble and I watch the world revolve around me from within it. No one sees my bubble, but it is there, a film deadening the noise and commotions of the world, as life goes on everywhere else. (Smith 2008, p.11)
Edwards’ painting clearly depicts an experience of ‘liminality’ (Sibbett 2004, 2005a, 2005b, 2005c) often expressed by people living with life-threatening and chronic illnesses. Liminality is described as a place where feelings of ‘limbo, ambiguity, embodied experience, chaos…expression and transition’ are manifest, as well as being a place of creativity and adaption where rites of passage are played out (Sibbett 2005a, p.68). What is characterised by Young’s (1988, p.22) quote is that people living with a diagnosis of life-threatening and chronic illness often find themselves suddenly, and earth shatteringly, transported into this liminal ‘betwixt and between’ threshold space (Sibbett 2004, 2005a, 2005b; Turner 1969), an unknown world or landscape without a ‘compass’ to guide them. It is a place where social stigma and ‘the sick role’ cause feelings of shame and distress, and people are described in passive terms as ‘dependent’ (Fraser and Gordon 1994) or ‘disabled’, thus further disrupting self-identity. My aim in developing portrait therapy is that the portraits created for patients will become points of reference within the journey into this unknown and liminal space (liminality will be discussed in more detail in Chapter 2).
Illness as unhomelike being-in-the-world
When researching the impact of chronic illness on self-identity I discovered the writings of university professor and philosopher Havi Carel (2004, 2007, 2008, 2011, 2012, 2014; Carel et al. 2016), who writes about her own experience of living with a chronic illness. Carel writes about being ‘unable to transcend the social barrier created by illness’ (2008, p.50), about a ‘bitterness’ which is ‘verboten’, and the pressures of being manoeuvred into being courageous and uncomplaining (ibid. p.55):
…first I am set up in a social context that forbids me from talking about my illness. Then, when I turn to other topics, I discover the social reward: I am seen as brave, graceful, a good sport… This is how you are seen once you conform to the demands and expectations of society: once your ‘sick role’ (as Talcott Parsons called it) is validated by those around you.
Carel (2008, p.50) also talks about how illness brings with it a distinct change in self-perception, which is mirrored by changes in social perception; she says:
…the thought that was truly novel for me was this: I will never get better. All the usual rules that governed my life – that trying hard yields results, that looking after yourself pays off, that practice makes perfect – seemed inoperative here. It was the first instance, for me, of unconditional, uncontrollable failure. No matter what I did, I would only get worse. The inevitability of decline was the only principle governing my life. (Carel 2008, p.63)
The disruption caused by illness also impacts upon the way patients think others perceive them:
…I became aware that I had fallen from a position of respect, friendship and admiration, to one of pity, pitied by all, admired by none. An instant and unwelcome change. Who am I now? (Smith 2008, p.7)
These accounts describe a double betrayal by the body, first in becoming the container for ‘disease’ and second in ‘revealing’ that disease, through the dysfunction and dis-ability of the body.
Bodies which have been compromised by illness also change how life is experienced, which can result in a profound disruption to a person’s sense of self (Carel 2011, p.36). The French phenomenological philosopher Merleau-Ponty (1908–1961) wrote extensively about how the body is central to the way we perceive experience and interpret the world, indeed, he believed that it is the whole reason we have a world to experience (Matthews 2006; Merleau-Ponty 2002). Portrait therapy therefore recognises the importance of the body in our experience of self-identity, and the embodied nature of all experience, especially within the experience of illness which can lead to feelings of ‘unhomelikeness’ (Svenaeus 2011, p.334).
Fredrik Svenaeus (professor of medical humanities and philosophy at Södertörn University, Sweden) has developed a phenomenological model of illness within which he defines the ‘otherness’ of the ill-body and the ‘enforced inhabitation of an alien world’ as ‘unhomelikeness’ (2011, p.334). He believes that diseases and the over-medicalisation and objectification of the body are therefore a direct threat to our ‘homelike being-in-the-world’, through their ‘radical and dreadful otherness’ (Svenaeus 2011, p.335).
…the unhomelike being-in-the-world of illness, in contrast to other forms of unhomelike being-in-the-world is characterized by a fatal change in the meaning-structures, not only of the world, but of the self… (Svenaeus 2011, p.337)
Within his seminal thesis on identity, philosopher Charles Taylor (1989) suggests that we all have a fundamental need for a sense of meaning in our lives. However, one of the key changes in thinking around self-i...