![]()
Brain, Nerves and Senses
![]()
Chapter
22
An Approach to Headache
Clinical Case
A 50-year-old office manager presents with a severe headache (pain score 10/10). She was having a bad day in the office when a severe headache suddenly started 6 hr ago. She has had headaches in the past but none this bad. Her only other past medical history is hypertension, for which she had defaulted medications. A CT Brain, performed 1 hr ago in the Emergency Department, is normal. She feels much better after having been given paracetamol and diclofenac in the Emergency Department, and asks if you could discharge her now. Would you agree?
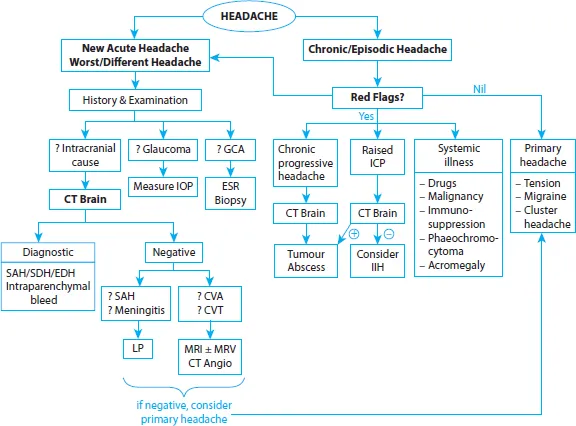
Many people have occasional headaches, and live with them, with little consequence. Yet some headaches can be life-threatening. Begin by characterising the headache’s time course. A patient who has had a particular episodic headache for years probably won’t be harmed by that headache. Conversely, the patient with his first-ever severe headache, or the patient who has a headache 10 times worse than his usual migraine, is far more likely to have a sinister cause of headache. Figure 22.1 provides an approach.
New Acute Headache
A number of neurologic emergencies present as a new acute headache. As patients with known migraine can also develop an unrelated neurologic emergency, any unusually severe headache or headache of a different character should also be investigated as a ‘new’ headache.
History and Examination
The clinical picture is often characteristic. Intracranial causes:
•Meningitis: An unwell patient with fever, neck stiffness and photophobia. Examination reveals nuchal rigidity (resistance to passive flexion), Kernig’s and Brudzinski’s signs, and may show a non-blanchable purpuric rash (in meningococcaemia). Bacterial meningitis presents over hours to a day, while fungal and tuberculous meningitis may present in a more subacute fashion.
•Subarachnoid haemorrhage (SAH): Classically, ‘the worst headache in my life’—sudden onset with pain maximal within seconds to minutes, but improving after. Patients may misleadingly be pain-free by the time of consult, or still have nuchal rigidity. It is important to diagnose SAH—catastrophic rupture of an intracranial aneurysm is imminently preventable.
CVA, cerebrovascular accident; CVT, cerebral venous thrombosis; EDH, extradural haemorrhage; ESR, erythrocyte sedimentation rate; GCA, giant cell arthritis; IIH, idiopathic intracranial hypertension; IOP, intraocular pressure; LP, lumbar puncture; MRV, magnetic resonance venogram; SAH, subarachnoid haemorrhage; SDH, subdural haemorrhage.
Figure 22.1. Approach to headache.
•Subdural haemorrhage (SDH): Typically, an elderly patient who sustains head trauma and subsequently develops headache within days (acute SDH) or weeks (chronic SDH). There may also be drowsiness or subtle confusion, localising neurological deficits and vomiting (due to raised intracranial pressure). The history of trauma may be remote and minor, especially in the elderly.
•Extradural haemorrhage (EDH): Usually a younger patient who suffered head trauma (e.g., a road traffic accident).
•Cerebrovascular accident: While most strokes do not present with headache, headache can occur in (a) some haemorrhagic strokes, (b) occipital strokes and (c) carotid dissection. A history of headache on exertion, or the presence of any neurological deficit (including an isolated Horner’s syndrome, which may occur in carotid dissection) increases the suspicion for stroke.
•Cerebral venous thrombosis (CVT): Usually occurs in females with a hypercoagulable state (including pregnancy and oral contraceptive pills). Presentation is variable; in addition to headache, there may be symptoms of raised intracranial pressure (ICP) (e.g., vomiting), seizure or neurological deficit.
Referred pain: Two causes of referred pain require emergent treatment—these must be identified on history and examination, not CT brain. | Workup |
•Acute closed-angle glaucoma: Unilateral headache ± vomiting with severe eye pain, blurring of vision and halos around lights. Eye is red with a fixed, mid-dilated pupil. A relative afferent pupillary defect can be seen if the optic nerve is damaged. Urgent treatment prevents blindness. | –Measure intra-ocular pressure, for example, Goldmann tonometry |
•Giant cell arteritis (temporal arteritis): Unilateral headache with jaw claudication (jaw pain when chewing), transient visual loss or visual field defect and scalp tenderness. There may be systemic symptoms of polymyalgia rheumatica (joint pains, peripheral synovitis, constitutional symptoms). Examination may find visual field defect and optic disk swelling. This is an autoimmune disease usually in > 50 year olds; early treatment prevents visual loss. | –ESR: usually high –Confirmation via temporal artery biopsy (but do not wait to start treatment, and beware of a falsely normal biopsy due to skip lesions) |
Intracranial Causes: Upfront CT Brain
Suspicion of a dangerous intracranial process generally justifies a plain CT brain upfront. This provides important diagnostic information and facilitates further investigations (e.g., excludes mass lesions so that lumbar puncture can be performed safely).
–Positive CT Brain: CT brain is particularly sensitive for intracranial haemorrhage, which appears white on CT (Figure 22.2).
–Negative CT Brain: CT brain is generally negative in meningitis, and may be negative in CVT, small SAH and early or minor stroke. Proceed based on the likely working diagnosis (a) suspected SAH or meningitis, or (b) suspected stroke or CVT.
Further Investigation: (a) Suspect SAH or Meningitis
Lumbar puncture is the next test if SAH or meningitis is suspected.
In suspected SAH: The sensitivity of CT...