An accessible and engaging review of board exam essentials
Cardiology Board Review lays the groundwork for board exam success with its instructive and easy-to-read explanations of the pathophysiology, diagnosis, and treatment of patients with cardiovascular disease. Breaking topics down into case ?unknowns,? this innovative revision aid provides examples of everyday cardiological issues and then explains how best to address the problem at hand. All content is complemented by clinical images and illustrations, as well as helpful summaries and key points.
Featuring 56 different cases, this essential text:
- Places learning in a practical context. Information about disease states is presented in case-based format which leads to better retention.
- Covers topics including congenital heart disease, coronary artery disease, cardiomyopathies, valvular heart disease, arrhythmias, heart failure, peripheral vascular disease, and more
- Designed to present important concepts and information in a unique way to complement textbook learning
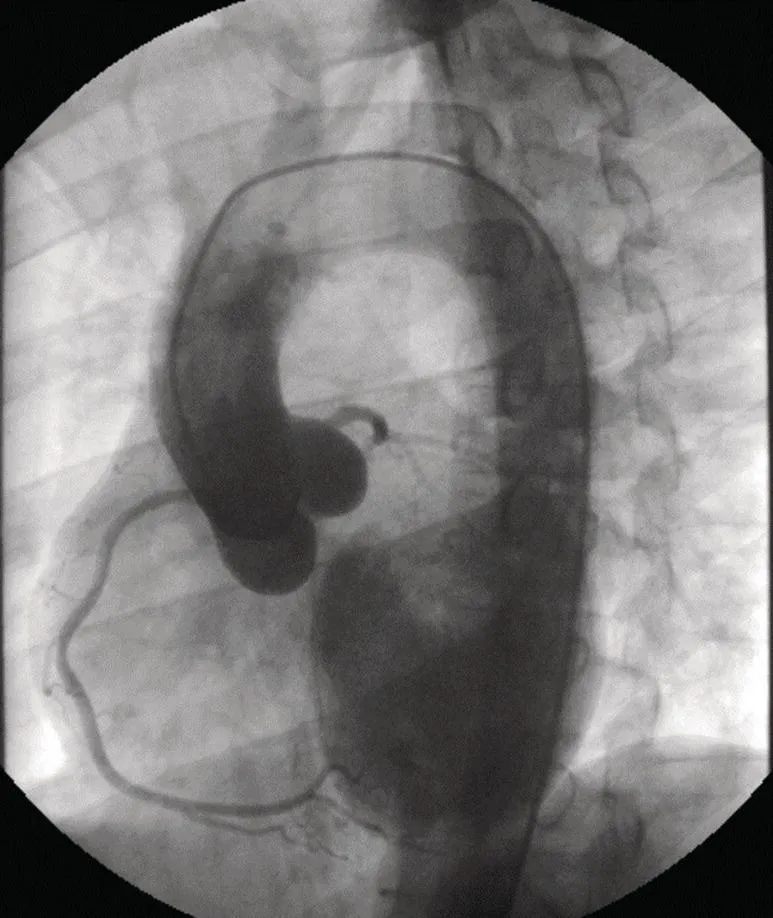
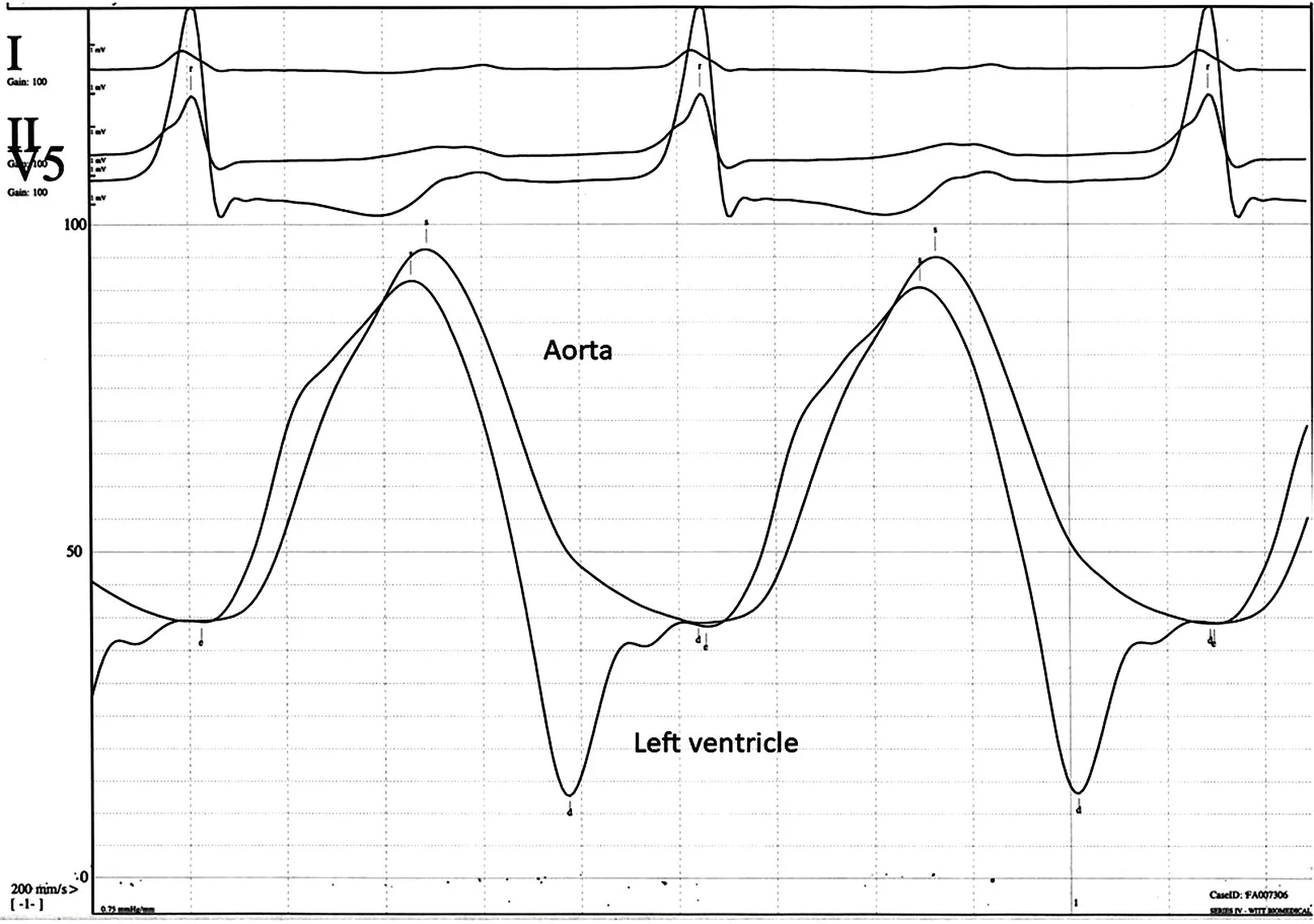
- Features electrocardiograms, angiograms, and pressure tracings
- Is applicable to those working towards certification in Cardiovascular Disease from the American Board of Internal Medicine or preparing for board examinations in other countries
- Is also suitable for those requiring MOC recertification
- Features cases on aortic insufficiency, atrial fibrillation, Brugada syndrome, carotid artery disease, myocardial bridging, congenital heart disease, electrolyte abnormalities, apical HCM, mitral regurgitation, RV outflow tract tachycardia, pulmonary hypertension, arrhythmogenic right ventricular dysplasia, aortic stenosis, atrial myxoma, atrial tachycardia, pulmonic insufficiency, Takotsubo, tricuspid regurgitation, Wolfe-Parkinson-White syndrome, pulmonic stenosis, coronary anomalies, ECG changes of hypothermia, endocarditis, pulmonary embolus, ventricular septal defect, hemodynamics of hypertrophic cardiomyopathy, complete heart block, heart failure, coronary artery disease, atrial septal defect, constrictive pericarditis, fractional flow reserve, dextrocardia, STEMI, early repolarization, giant cell myocarditis, peripheral arterial disease, pericardial tamponade, peripheral arterial disease, pericarditis, myocarditis, long QT syndrome, mitral stenosis, tetralogy of Fallot, and supraventricular tachycardia among others.
Cardiology Board Review offers fellows a fresh and engaging approach to the information required to achieve success in board examinations.