From the publishers of the market-leading at a Glance series comes a comprehensive yet accessible overview of all the fundamental elements of acute and critical care nursing.
Acute and Critical Care Nursing at a Glance provides an introduction to the key knowledge and skills for patient assessment and problem identification, as well as how to plan, implement and evaluate care management strategies. It also explores clinical decision-making processes and their impact on care delivery, as well as key psychosocial issues, pain management, and safe transfer. All information is presented in a clear, double-page spread with key information accompanied by tables, illustrations, photographs and diagrams.
Key features:
- Superbly illustrated, with full colour illustrations throughout
- An accessible, evidence-based, introduction to a complex topic
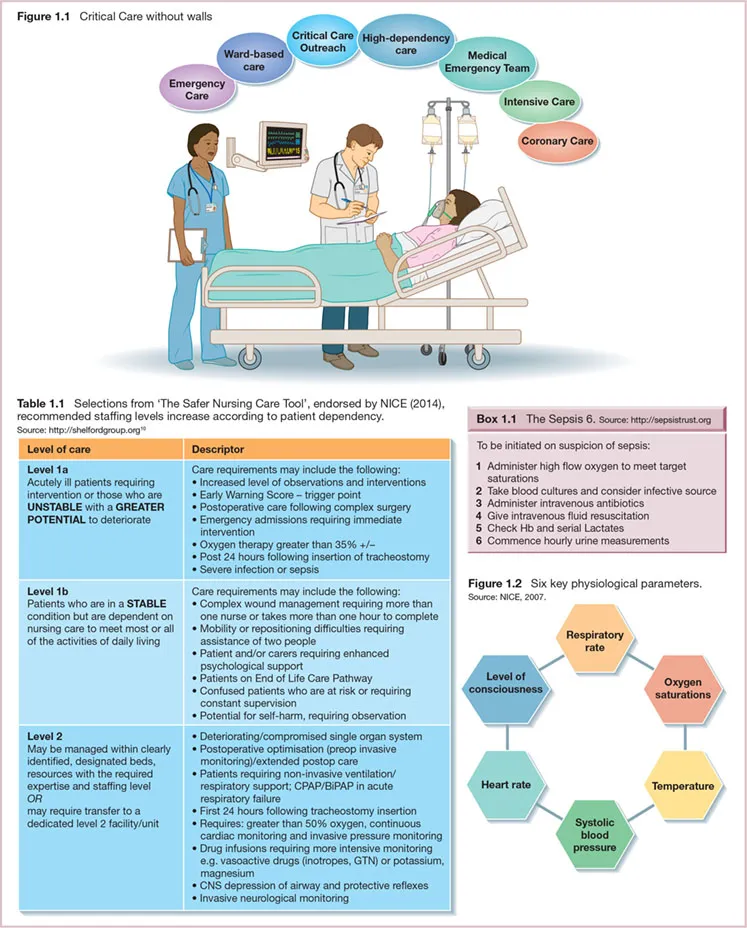
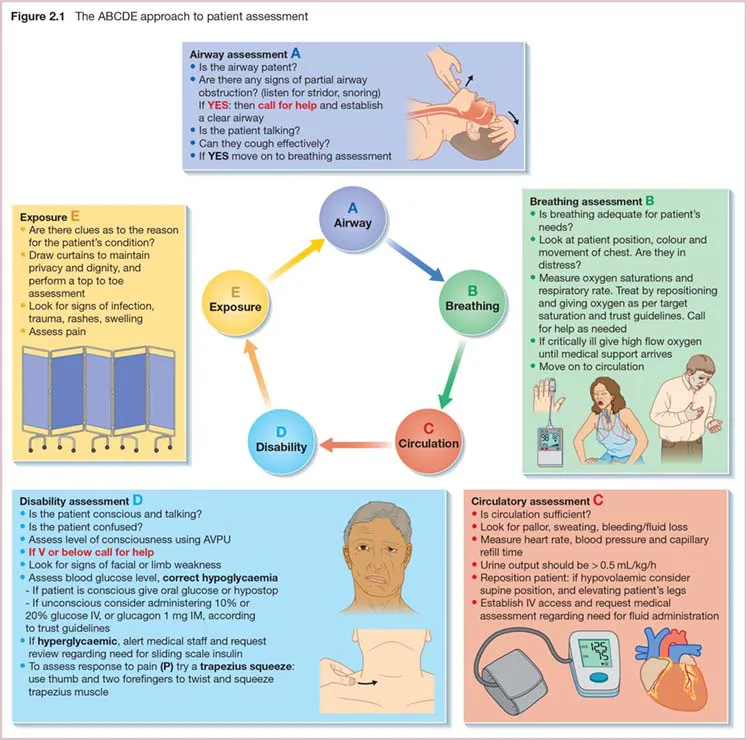
- Presents information structured according to the Resuscitation Council's systematic ABCDE framework for ease of understanding
- Accompanied by patient case studies to help apply theory to practice
Acute and Critical Care Nursing at a Glance is ideal for nursing students, healthcare assistants, and registered nurses working within the acute and critical care setting.