Botulinum Toxins: Cosmetic and Clinical Applications provides a comprehensive and in-depth review of the use of botulinum toxin for aesthetic procedures and medical applications as a stand-alone treatment and as part of combination therapy.
Now a mainstay of cosmetic dermatologic practice, the range of available toxins and their varied applications has grown considerably in recent years requiring the practitioner to carefully consider what approach best suits the needs of their patient. This new book, written by international expert authors, provides guidance to help you refine your technique, add new procedures to your practice, and provide optimal results.
This book:
Offers guidance on best-practice approaches with botulinum toxin, helping create cutting edge, tailored treatment plans for each patient
Benefits from a wealth of color images, procedural videos, and expert tips and tricks
Takes a region oriented approach, providing guidance on treatment of the; glabella, forehead, periocular and perioral areas, and contouring of the lower face and lower leg and calf, and neck rejuvenation
Contains a thorough review of non-cosmetic treatments such as correction of facial asymmetry, and treatment of axillary hyperhidrosis, plus palm, sole, and craniofacial hyperhidrosis
Covers exciting new topics, such as future injectables, topical botulinum toxin, and facial contouring including treatment for benign masseter hypertrophy
Discusses combination therapy of botulinum toxin with other non-surgical procedures such as hyaluronic acid (HA) or filler substances, light and laser sources, and other energy-based therapies
Includes considerations for darker skin types
Offer your patients the best care, stay on top of cutting edge techniques, and avoid pitfalls with coverage of practical tips and real cases. Botulinum Toxins in Dermatology: Cosmetic and Clinical Applications provides best-practice guidance on the contemporary use of botulinum toxin in isolation and in combination.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1 History of Botulinum Toxin for Medical and Aesthetic Use
Alastair Carruthers,FRCPC1 and Jean Carruthers, MD (FRCS(C), FRCOphth)2
1 Clinical Professor, Department of Dermatology and Skin Science, University of British Columbia, Vancouver, Canada
2 Clinical Professor, Department of Ophthalmology and Visual Sciences, University of British Columbia, Vancouver, Canada
Sausage Poisoning
In the late 1700s in Europe, outbreaks of a deadly illness from contaminated foods swept across the continent, fueled in part by the poverty from the Napoleonic War (1795–1815) that led to unsanitary food production [1]. The primary source of food-borne illness of the time: smoked blood sausages. One of the biggest outbreaks occurred in 1793 in Wildebrad, Southern Germany; by 1811, the Department of Internal Affairs of the Kingdom of Würtemberg named “prussic acid” as the culprit in sausage poisoning [2]. Intrigued, the district medical officer and poet, Dr. Justinus “Würst” Kerner (1786–1862), began what would become a lifelong quest to uncover the mysteries of the poison. He would later be considered the godfather of botulinum toxin (BoNT) research for his early, intensive work. In 1817 and 1820, Kerner identified and described the first accurate descriptions of botulism (a term coined in 1871 from the Latin botulus, meaning “sausage”) [2, 3]. In 1822, he compared contaminated sausage ingredients and concluded that the toxin must occur in fat, leading him to call the suspicious substance “sausage poison,” “fat poison,” or “fatty acid,” and published the first complete monograph of the “fatty toxin” from blood sausages [2].
In his monograph, Kerner described the symptoms of botulism – including vomiting, intestinal spasms, mydriasis, ptosis, dysphagia, and respiratory failure – and recommended methods for the treatment and prevention of food poisoning. Through animal and self-experimentation, Kerner observed that the toxin developed under anaerobic conditions and was lethal in small doses. Since the effects of this blood poison were similar to atropine, scopolamine, nicotine, and snake venom, Kerner surmised that sausage poison was likely biological in nature – remarkable in that microscopic pathogens had not yet been discovered at that time – and interrupted signal transmissions within the peripheral and autonomic nervous system. Indeed, some would call Kerner prophetic: he suggested that small amounts of this sausage poison might be used to lower sympathetic nervous system activity associated with movement disorders (i.e., treat St. Vitus' dance or Sydenham's chorea, a disorder characterized by jerky, uncontrollable movements, either of the face or of the arms and legs) and hypersecretion of bodily fluid, as well as to treat ulcers, delusions, rabies, plague, tuberculosis, and yellow fever [4].
Identification of C. botulinum
Microbiologist Professor Emile Pierre van Ermengem (1851–1922) trained under Robert Koch, who discovered anthrax, tuberculosis, and cholera and was the first researcher to prove that microorganisms could cause disease in animals [5]. In 1897, Van Ermengem identified the bacterium Clostridium botulinum (originally called Bacillus botulinus) as the causative agent of botulism after examining postmortem tissue of patients in Belgium who had contracted gastroenteritis and died from eating raw, salted pork [6]. Over the next twenty years, different strains of the bacterium that produced serologically distinct types of toxins were recognized; these were eventually classified alphabetically into seven serotypes (A, B, C1, D, E, F and G) [7]. In 1928, Dr. Herman Sommer (University of California, San Francisco) isolated the most potent serotype – BoNT type A (BoNTA) – in purified form as a stable acid precipitate, paving the way for future studies [8].
Biological Weapon of Warfare
During the First World War, Germany unsuccessfully attempted to produce chemical and biological weapons. As World War II approached, the American government learned that multiple countries were engaged in bio-warfare programs. In response, and on orders from President Franklin Roosevelt, the US National Academy of Sciences and Fred Ira Baldwin, chairman of the bacteriology department of the University of Wisconsin, gathered bacteriologists and physicians in a laboratory named Fort Detrick (Maryland). The purpose of Fort Detrick: the investigation of dangerous infectious bacteria and toxins to use as offensive and defensive biological weapons [1].
In 1946, Carl Lamanna and James Duff developed concentration and crystallization techniques for the toxin that were subsequently used by Dr. Edward J. Schantz, a young US army officer stationed at Fort Detrick to produce the first BoNTA lot for human use (the basis of the later clinical product) [9, 10]. The US Office of Strategic Services (OSS) developed a plan using Chinese prostitutes to assassinate high-ranking Japanese officials via gelatin capsules containing the newly purified BoNTA. The government abandoned the plan when test donkeys that received the capsules survived [1]. Ironically, though BoNT today is considered one of the deadliest poisons in the world – 1 g has the potential to kill 1 million people – the toxin is not an ideal biological weapon, since large amounts must be ingested and mortality rates vary).
In 1972, President Richard Nixon signed the Biological and Toxic Weapons Convention, effectively putting an end to all investigations on biological agents for use in war. Schantz took his research to the University of Wisconsin, where he produced a large amount of BoNTA (batch 79–11) that remained in clinical use until December of 1997 [11].
Human Experimentation
Clinical use of the toxin began in the late 1960s and early 1970s, when Dr. Alan Scott (Smith-Kettlewell Eye Research Foundation, San Francisco; Figure 1.1) began experimenting with BoNTA, supplied by Dr. Schantz, and other chemical agents in monkeys, with the hope that one of the compounds could be used for the nonsurgical treatment of strabismus in humans [12, 13]. Scott published his first primate studies proving that BoNTA could weaken extraocular muscles in 1973, and postulated that the toxin could be used for a wide variety of musculoskeletal disorders and spasticity, even before conducting any human studies [13, 14]. In 1978, Scott received Food and Drug Association (FDA) approval to begin testing small amounts of the toxin (then named Oculinum) in human volunteers; his landmark paper, published in 1980 [15], showed that intramuscular injections of BoNTA could correct gaze misalignment in humans. In 1989, one year after manufacturer Allergan Inc. (Irvine, CA) acquired the rights to distribute Scott's Oculinum in the United States, BoNTA was approved for the nonsurgical correction of strabismus, blepharospasm, hemifacial spasm, and Meige's syndrome in adults, and clinical use expanded to include the treatment of cervical dystonia and spasmodic torticollis [13, 16, 17]. Shortly thereafter, Allergan bought Scott's company and renamed the toxin. Botox® was born.
Figure 1.1 Dr Alan Scott, the original user of botulinum toxin A initially in monkeys and then in humans, seen in 2010.
The Cosmetic Connection
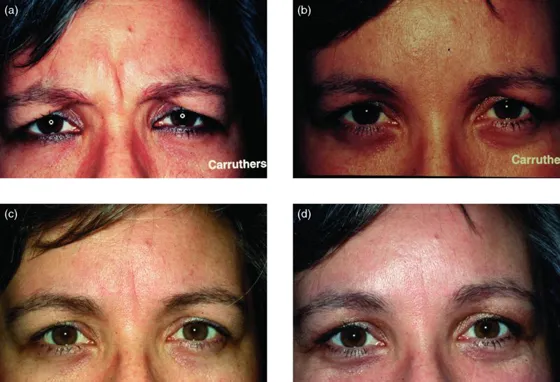
In the mid-1980s, Dr. Jean Carruthers, an ophthalmologist in Vancouver, Canada, noticed that her patients injected with BoNTA for blepharospasm experienced a reduction in glabellar rhytides, and discussed the findings with both Scott and her dermatologist spouse, Dr. Alastair Carruthers, who was attempting to soften the forehead wrinkles of his patients using soft-tissue augmenting agents available at that time. Intrigued by the possibilities, the Carruthers used the toxin experimentally in their receptionist's forehead and subsequently published the first report of BoNTA for the treatment of glabellar frown lines in 1992 [18] (Figure 1.2). Other reports soon followed [19, 20], including the first double-blind, placebo-controlled study for the treatment of hyperkinetic facial lines [21].
Figure 1.2 The Carruthers' first patient treated in the glabella area for cosmetic reasons alone. Seen (a) before frowning; (b) after frowning; (c) before at rest; (d) after at rest.
Properties, Mechanism of Action, and Clinical Effect
Clostridium botulinum is a rod-shaped, gram-positive anaerobic bacterium. Of the seven serotypes, A, B, and E are commonly involved in human botulism [22]. BoNT is a high-molecular-weight protein of 150,000 daltons with nonconvalent proteins protecting it from digestive enzymes, making it a lethal cause of food poisoning [1]. The symptoms of botulism include disturbances in vision, speech, and swallowing, with asphyxia and death sometimes occurring 18–36 hours after ingestion (mortality rate: 10–65%) [22].
Researchers gained an understanding of mechanism of action in the late 1940s, when they discovered that BoNT blocks neurotransmitter release at the neuromuscular junction [23]. The follow-up discovery in the mid-1950s that BoNT blocks the release of acetylcholine from motor nerve endings...
Table of contents
Cover
Title page
Copyright
List of Contributors
About the Companion Website
Video Table of Contents
Foreword: Botulinum Toxins in Dermatology
1 History of Botulinum Toxin for Medical and Aesthetic Use
2 Anatomy and Aesthetic Principles
3 Botulinum Toxin: From Molecule to Medicine
4 Myobloc
5 Abobotulinumtoxin: Development and Aesthetic Usage
6 IncobotulinumtoxinA (Xeomin®/Bocouture®)
7 Future Injectable Toxins
8 Reconstitution, Dilution, Diffusion, and Migration of Botulinum Toxin
9 Patient Selection
10 Treatment of the Glabella
11 Treatment of the Forehead
12 Treatment of the Periocular Area – Crow's Feet, Brow, and Bunny Lines
13 Contouring of the Lower Face and of the Lower Leg and Calf
14 Treatment of the Perioral Area
15 Neck Rejuvenation
16 Correction of Facial Asymmetry
17 Complications and Diffusion
18 Combination Therapy of Botulinum Toxin with other Nonsurgical Procedures
19 Peri-Procedure Botulinum Toxin for Skin Cancer Patients and Scars
20 Achieving a Natural Look
21 Special Considerations in Darker Skin
22 Axillary Hyperhidrosis
23 Primary Focal Palm, Sole, Craniofacial, and Compensatory Hyperhidrosis
24 Topical Botulinum Toxin
25 Exciting New Uses of Botulinum Toxin Type A: Dermatology/Dermatologic Surgery and Beyond
26 Modulating Affect and Mood with Botulinum Toxin Injections: Psychosocial Implications of Neuromodulators
27 OnabotulinumtoxinA (Botox®) in Dermatology
Index
EULA
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Botulinum Toxins by Joel L. Cohen, David M. Ozog, Dennis A. Porto, Joel L. Cohen,David M. Ozog,Dennis A. Porto in PDF and/or ePUB format, as well as other popular books in Medicine & Dermatology. We have over 1.5 million books available in our catalogue for you to explore.