- English
- ePUB (mobile friendly)
- Available on iOS & Android
Clinical Reproductive Science
About this book
The comprehensive and authoritative guide to clinical reproductive science
The field of clinical reproductive science continues to evolve; this important resource offers the basics of reproductive biology as well as the most recent advance in clinical embryology. The author - a noted expert in the field - focuses on the discipline and covers all aspects of this field. The text explores causes of male and female infertility and includes information on patient consultation and assessment, gamete retrieval and preparation, embryo culture, embryo transfer and cryopreservation.
Comprehensive in scope, the text contains an introduction to the field of clinical reproductive science and a review of assisted reproductive technology. The author includes information on a wide range of topics such as gonadal development, the regulation of meiotic cell cycle, the biology of sperm and spermatogenesis, in vitro culture, embryo transfer techniques, fundamentals of fertilisation, oocyte activation and much more. This important resource:
- Offers an accessible guide to the most current research and techniques to the science of clinical reproduction
- Covers the fundamental elements of reproductive science
- Includes information on male and the female reproductive basics – everything from sexual differentiation to foetal development and parturition
- Explores the long-term health of children conceived through IVF
- Contains the newest developments in assisted reproductive technology
Clinical Reproductive Science is a valuable reference written for professionals in academia, research and clinical professionals working in the field of reproductive science, clinical embryology and reproductive medicine.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Section Three
Clinical Reproductive Science In Practice: IVF and Assisted Reproductive Technologies
18
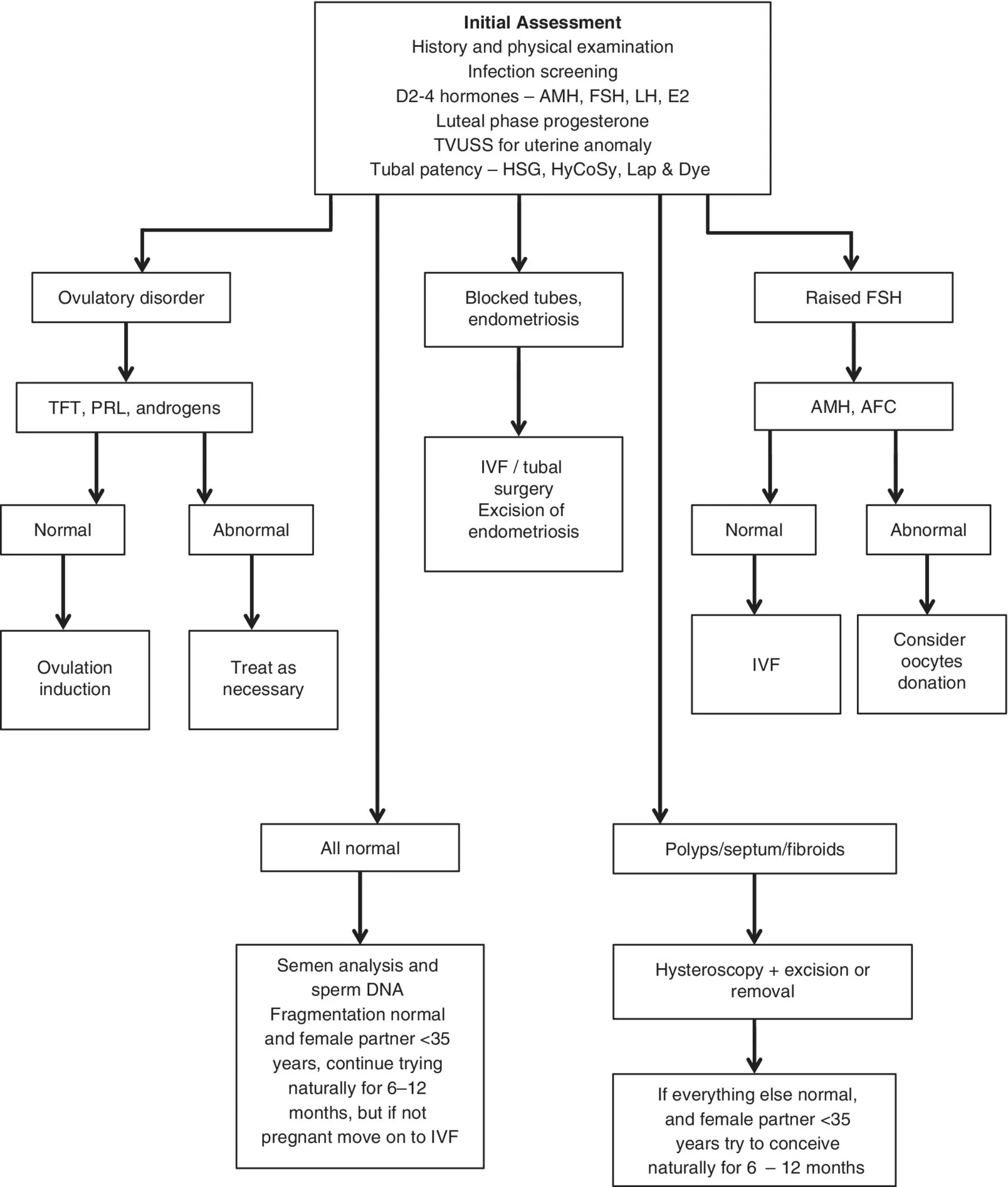
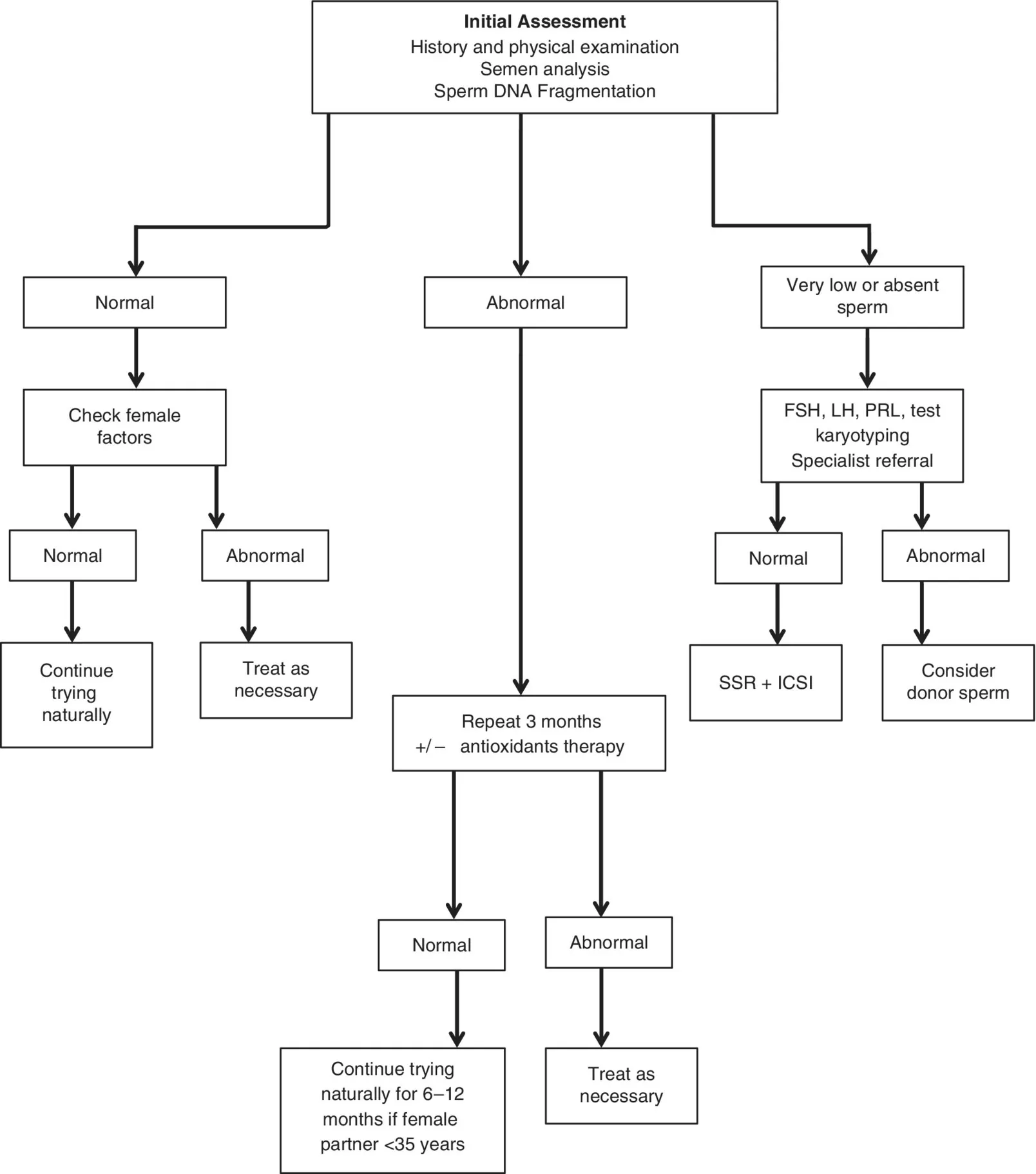
Assessing the Infertile Couple
Introduction
Definitions
- Infertility is defined as the inability to conceive after regular unprotected sexual intercourse for 12 consecutive months, in the absence of any known cause (NICE 2013).
- Subfertility is defined as the inability to conceive due to reduced fertility. Clear understanding of the definitions of sub‐ and infertility is very important for the appropriate management of infertility (Gnoth et al. 2005).
- Primary infertility is when someone has never conceived in the past and has difficulty conceiving now.
- Secondary infertility is when someone has had one or more pregnancies in the past and has difficulty conceiving now.
Epidemiology of Infertility
History Taking: Female Partner
- Woman aged over 35 years
- No previous pregnancy
- Trying to conceive for >3 years
- Infrequent sexual intercourse
- Woman’s body mass index (BMI) <20 or >30
- Regular use of recreational drugs
- Sexually transmitted infections
- Lifestyle factors including smoking in one or both partners, caffeine intake >2 cups of coffee per day.
- Menstrual history: age of menarche, cycle characteristics – frequency, duration, dysmenorrhoea, intermenstrual or postcoital bleeding. Review for any history of primary or secondary amenorrhoea. Women with regular menstrual cycles are very likely to be ovulating and should be reassured.
- Obstetric history: previous pregnancies, if any, and its outcome, recurrent pregnancy loss, terminations, infection or puerperal sepsis.
- Contraceptive history: previous use of contraceptives, any associated problems including lost coil, latest contraceptive methods and when last used. This is particularly relevant for medroxyprogesterone injections and combined pills as the return of fertility can be longer –up to 1 year in some cases.
- Sexual history: frequency of intercourse, timing in relation to the cycle, use of vaginal lubricants, douching after sexual intercourse, dyspareunia, loss of libido, and history of any sexually transmitted infections
- Medical history: diabetes, hypertension, thyroid disorder, cystic fibrosis, sickle cell disease, tuberculosis, and history of ovarian cysts. Enquire about rubella status.
- Surgical history: appendicectomy, tubal surgery, pelvic surgery, laparotomy and bowel surgery, Caesarean sections, and cervical loop excision or conization.
- Family history: consanguinity, diabetes mellitus, hypertension, and cancer.
- Social history: occupation, diet, drug history including recreational drugs such as marijuana and cocaine, smoking, alcohol and caffeine consumption.
| Causes of Female ... |
Table of contents
- Cover
- Table of Contents
- About the Editor
- Preface
- Section One: Reproductive Science
- Section Two: Clinical Reproductive Science
- Section Three: Clinical Reproductive Science In Practice
- Index
- End User License Agreement
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app