Written by an experienced and well-respected physician and professor, this new volume, building on the previous volume, Ultrasonic Topographical and Pathotopographical Anatomy, also available from Wiley-Scrivener, presents the ultrasonic topographical and pathotopographical anatomy of the head and neck, offering further detail into these important areas for use by medical professionals.
This atlas of topographic and pathotopographic human anatomy is a fundamental and practically important book designed for doctors of all specializations and students of medical schools. Here you can find almost everything that is connected with the topographic and pathotopographic human anatomy, including original graphs of logical structures of topographic anatomy and development of congenital abnormalities, topography of different areas in layers, pathotopography, computer and magnetic resonance imaging (MRI) of topographic and pathotopographic anatomy. Also you can find here new theoretical and practical sections of topographic anatomy developed by the author himself which are published for the first time. They are practically important for mastering the technique of operative interventions and denying possibility of iatrogenic complications during operations.
This important new volume will be valuable to physicians, junior physicians, medical residents, lecturers in medicine, and medical students alike, either as a textbook or as a reference. It is a must-have for any physician's library.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Limits, outer orienteers. The head is separated from the neck with the line which begins on chin elevation – protuberantia mentalis, after that it laterally continues across the lower mandible edge, continues by the lower semicircle of outer aural meatus, goes on to the upper nuchal line, linea nuchae superior, and ends on both sides on outer elevation of occipital bone with protuberantia occipitalis externa. In general, the head is divided into cerebral cranium – cranium cerebrale and facial cranium – cranium faciale.
Cerebral Cranium
Limits: The cerebral cranium is separated from facial cranium with the anatomical formations described below. It is limited by glabella by the middle line. Afterwards this line goes along the brow arch, arcus superciliaris, then - by the rear edge of the processus zygomaticus ossis frontalis and processus frontosphenoidalis ossis zygomatici, then the line goes on by the zygomatic arch, then it continues vertically to the rear edge of the ascending branch of the mandible, and afterwards it continues on the bottom margin where it ends after connecting with a similar line coming from the opposite side – forming protuberantia mentalis.
Area division: The cerebral cranium can be divided into the cranium base, basis cranii, and the cranium fornix (or dome) which is also called calvaria. The cranium base is divided into inner one (basis cranii interna) and external one (basis cranii externa). Calvaria is divided into frontal, parietal, occipital, temporal and mastoid regions (regg. Frontalis, parietalis, occipitalis, temporalis et mastoidea).
Regio frontalis (or the frontal area) is located within the frontal region. Its limiting line begins in the lower part of glabella, spreads to the sides across eyebrow arches, crosses the zygomatic process of the frontal bone, continues upwards across temporal line, and then ascends by the projection line of the coronal suture.
Regio parietalis (parietal region). Limits: anterior limit is the coronal suture, lambdoid suture is the rear limit, temporal line limits it from the sides.
Regio occipitalis (occipital region) is located within the squama of the occipital bone. Limits: lambdoid suture limits it from the top and from the sides and the line drawn horizontally from one apex of mastoid bone to another limits it from below. It’s called linea bimastoidea.
Regio temporalis (temporal region). Limits: upper and rear limit is the temporal line, lower limits are zygomatic arch and temporal line above the external aural canal, anterior limit is the zygomatic process of the frontal bone and the outer section of the temporal line. Layer topography of this area has its own complications: skin has less connective tissue septa the lower it is. Aponeurotic helmet becomes thinner and is called here fascia superficialis or superficial fascia. Fascia temporalis propria or proper temporal fascia is formed by the arcus zygomaticus after attaching with its lower margin. You can find its spatium interaponeuroticum, interaponeurotical space, between the plates.
Regio mastoidea or mastoid is an area which is limited with mastoid process. Layer topography of this area has its own complications: skin has no hair and is tightly attached with the mastoid aponeurosis or aponeurosis mastoideus lying below, which is a continuation of galea aponeurotica, but is significantly thinner that its origin. Mastoid process is covered with a thick layer of the periosteum and has attachment points of m. sternocleidomastoideus, mm. splenius capitis et cervicis, venter posterior m. digastrici.
Layers of Regions and their Characteristics:
Derma – thick, hair-covered skin, it has a large number of sebaceous and sweat glands. It is firmly attached to the deeper lying subcutaneous fat and supracranial muscle, musculus epicranius, using vertically going connective tissue septa.
Panniculus adiposus – it’s subcutaneous fat. Blood and lymphatic vessels of this layer are firmly fixed using connective tissue septa. That’s why vessels do not collapse when injured.
M. epicranius – it’s epicranius muscle which consists of the frontal part, m. frontalis, and the occipital part of the m. occipitatis. Both parts have shared tendon helmet, galea aponeurotica, which is located in the parietal region and becomes thinner as it goes laterally during transition to the temporal region. These three layers which were described above form a single layer of tightly interconnected tissues.
Stratum fasciaie – it’s fascial layer, a layer of incoherent connective tissue.
Periosteum is firmly attached to the skull bones only in the sutural areas.
Ossa cranii are the bones of the skull of variable thickness. Occipital region bones have the maximum thickness, and the temporal bones have the minimum thickness. The skull bones are composed of three layers. It’s the lamina externa or the external plate, substantia diploica or the spongeous matter which has a lot of vessels – especially vv. diploicae, and lamina vitrea or glass-like plate.
Spatium epidurale – it’s the space above the dura mater.
Dura mater is composed of dense fibrous connective tissue. As it goes deeper, this tunica forms the falx cerebri or the crescent of the brain and with its help it divides cerebral hemispheres from each other; falx cerebelli or the crescent of the cerebellum divides the cerebellar hemispheres, and tentonum cerebelli or the tent of the cerebellum separates the occipital lobes of the cerebral hemispheres from the cerebellum. These processes of dura mater form channels for the drainage of venous blood from the cranial cavity which are called venous sinuses.
Spatium subdurale is a space beneath the dura mater.
Arachnoidea encephali or the arachnoid membrane contains blood vessels and continues from one gyrus to another without going in.
Spatium subarachnoidaie or subarachnoid space stores cerebrospinal fluid in its subarachnoid cisterns or cisternae subarachnoidaie.
Pia mater or the soft tunica contains a large number of vessels. The tunica finds its way inside all the sutures between the gyruses.
Spatium epicerebrale or epicerebral space. Has the most amount of cerebrospinal liquid between all the listened above spaces.
Gyri cerebri or brain gyruses.
Regio Frontalis Has the Next Blood Vessels (Fig. 1):
a. frontalis is the final branch of the a. ophthatmica and leaves the cranial cavity through the frontal hole, for. frontale. A. frontalis anastomoses with the a. angularis in the corner of the eye;
a. suproorbitalis leaves the cranium through the incisura supraorbitalis. Frontal artery lies a little bit more medially than supraorbital. Venous backflow goes through the frontal veins, vv. frontales and after that backflow continues through v. angularis and afterwards it goes on to the system of frontal facial vein. A small amount of blood keeps going to v. ophthatmica superior which pours into the cavernous sinus.
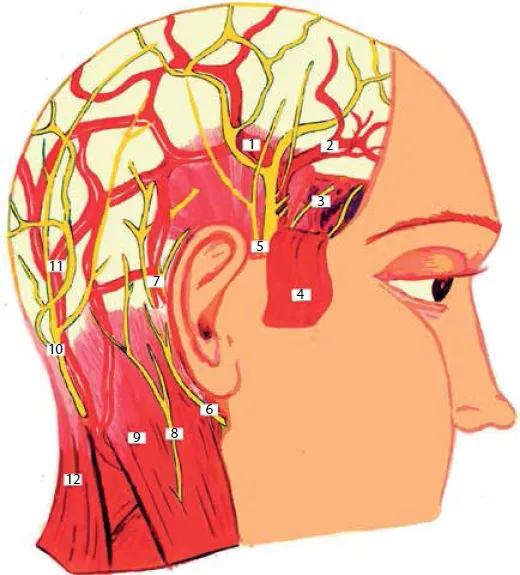
Figure 1 Vessels and nerves of the head.
1 – r. parietalis a. temporalis superficialis, 2 – r. frontalis a. temporalis superficialis, 3 – aa. et nn. temporales profundus, 4 – m. temporalis, 5 – n. auriculotemporalis, 6 – n. auricularis posterior, 7 – a. auricularis posterior, 8 – n. occipitalis minor, 9 – m. sternocleidomastoideus, 10 – n. occipitalis major, 11 – a. occipitalis, 12 – m. trapezius
Innervation: motor nerves of this region descend from ramus frontalis n. facialis; sensitive nerves – from ramus ophthalmicus n. trigemini. Lymph drainage of this area is performed through nodi auriculares anteriores, which are located a little a bit more forward than the tragus of the ear.
Regio parietalis is supplied with blood with r. parietalis a. temporalis superficialis. Venous backflow goes through r. parietalis v. temporalis superficialis. Innervation of the area: front is innervated with n. supraorbitalis and n. frontalis, sides – with n. auriculotemporatis, rear – with n. occipitalis major. Lymphatic backflow is supplied with nodi auriculares posteriores.
Regio occipitalis is supplied with blood through a. occipitalis, which branches off a. carotis externa. A. occipitalis gets under m. sternocleidomastoideus and comes close to v. jugularis interna and n. occipitalis minor. Terminal branches a. occipitalis are located under m. epicranius, where they diverge into rr. mastoidei, auriculares, occpitales. Venous outflow goes through the occipital vein, v. occipitalis which runs togethe...
Table of contents
Cover
Title page
Copyright page
About the Author
Introduction
Part 1: The Head
Part 2: The Neck
Appendix A
Appendix B
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Atlas of Topographical and Pathotopographical Anatomy of the Head and Neck by Z. M. Seagal in PDF and/or ePUB format, as well as other popular books in Medicina & Anatomía. We have over 1.5 million books available in our catalogue for you to explore.