- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Endodontology at a Glance
About this book
A practical and colourful introductory guide, Endodontology at a Glance covers all the essential topics (diagnosis, endodontic therapy, pain management and outcome of treatment) as well as the recent developments that comprise the field of endodontology. Written by experts in the field, the book explores the causes and sequelae of endodontic disease and offers suggestions for taking an effective patient history.
- New addition to the At a Glance series covering a core area of dentistry
- Review style makes for the ideal revision companion
- Includes access to a companion website with MCQs for self-assessment and downloadable images for use in teaching
Trusted by 375,005 students
Access to over 1 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part 1
Disease processes in endodontology
Chapters
- 1 The causes and sequelae of endodontic disease
- 2 Microbiology of apical periodontitis
- 3 Resorption
1
The causes and sequelae of endodontic disease
Pulpitis is the inflammation of the pulp, whereas apical periodontitis is the inflammation of the tissues surrounding the apex of the tooth, including the periodontal ligament and the alveolar bone. Inflammation can be acute or chronic.
Acute inflammation
Acute inflammation is characterised by:
- Redness
- Heat
- Swelling
- Pain
- Loss of function.
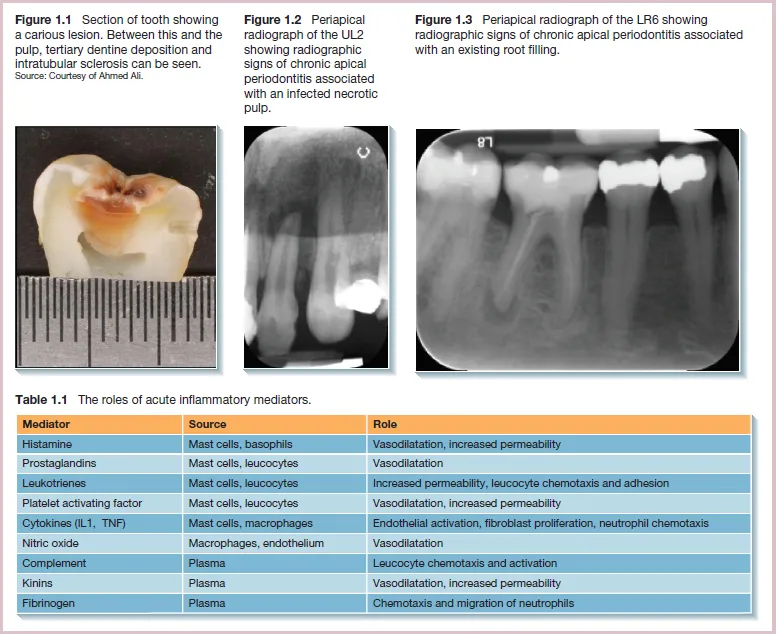
The redness and heat produced in an area of acute inflammation are the results of vessel dilatation and increased blood flow to that area. Swelling is caused by the accumulation of tissue exudates which contain neutrophils and inflammatory mediators (Table 1.1). The exudate aims to dilute the toxins whilst the neutrophils ingest the pathogens by phagocytosis. Pain is felt because of the swelling exerting pressure on nerve endings. Certain chemical mediators can also stimulate pain receptors. Swelling and pain can result in loss of function of the inflamed area.
Chronic inflammation
Acute inflammation can be reversible by removal of the damaging stimulus. However, if it persists, chronic inflammation ensues. Chronic inflammation is the result of a balance between continued tissue damage and attempts by the host to eradicate the disease to produce some tissue repair. Macrophages are among the main effector cells in chronic inflammation. They secrete various inflammatory mediators and have a role in phagocytosis and antigen presentation. Lymphocytes additionally recognise foreign antigens by binding to them before proliferating to mount an immune response by cell-mediated immunity (T lymphocytes) or by humoral immunity (B lymphocytes). Symptoms are usually limited at the chronic inflammation stage.
Causes of apical periodontitis
Apical periodontitis is caused by bacterial infection of the pulp. In a healthy tooth, the pulp dentine complex is protected from oral microorganisms by the overlying enamel and cementum. However, these layers can be damaged by caries, cracks or fractures, tooth wear, restorative procedures or periodontal procedures to produce portals of entry for microorganisms.
As bacteria penetrate into dentine, they release toxins that pass through the dentine tubules. The pulp responds to this by producing a layer of tertiary dentine as an additional protective layer. Increased intratubular mineral deposition may also reduce the permeability of the dentine (Figure 1.1). However, once the microorganisms penetrate into the inner dentine layers, the toxins they produce cause significant pulpal inflammation. If no treatment is provided, the bacteria eventually invade and colonise the pulp. The pulp is encased in a hard dentine shell and can therefore not expand to accommodate large amounts of fluid exudate. It also lacks sufficient collateral circulation. These factors limit the ability of the pulp to respond effectively to the insult. Pulpal inflammation can initially be reversible, with removal of the irritants resulting in resolution of the inflammation. However, as the immune challenge increases, the pulpal damage will advance beyond repair, resulting in irreversible inflammation and progressive pulpal necrosis.
Restorative procedures additionally may ‘push’ a tooth with pre-existing pulpal inflammation to irreversible pulpitis. This occurs by overheating, desiccation or chemical irritation to the dentino-pulp complex. If rubber dam is not used, or poor fitting temporary restorations are placed, microleakage can also occur. The risk of permanent damage is higher when the restorative work is close to the pulp and the dentine is permeable.
A root canal with a necrotic pulp is the ideal environment for bacterial colonisation as it provides a warm, moist, nutritious and anaerobic environment. The reduced presence of oxygen can also select aggressive anaerobic pathogens. The microorganisms are protected from the host defences as there is no blood circulation in the necrotic tissue. They derive their nutrients from the necrotic pulp tissue, periradicular tissue fluids, saliva and metabolic by-products of other bacterial species.
Over time, the bacteria progress apically down the root canal. Leakage of toxins and metabolic by-products through the apical foramen also stimulates the inflammatory response in the periapical tissues. Inflammatory mediators are released that stimulate osteoclast differentiation. This results in apical bone resorption and production of an apical lesion surrounded by chronic inflammatory cells. This stage of the disease is described as chronic apical periodontitis associated with an infected necrotic tooth (Figure 1.2).
The aim of root canal treatment is to reduce the bacterial load and seal the canals to prevent further ingress of bacteria. However, chronic inflammation can persist if inadequate disinfection is performed, with microorganisms remaining at levels sufficient to stimulate an inflammatory response. If the root canal system and coronal aspect of the tooth are not adequately sealed after root canal treatment, bacteria can re-enter and cause recurrence of the apical inflammation. It can be difficult to identify if the cause of the inflammation is persistence of, or re-entry of bacteria (or both). This stage of the disease is described as chronic apical periodontitis associated with an infected root-filled tooth (Figure 1.3).
Bacteria can egress through the apical foramen and, in some cases, cause suppuration that presents as an acute apical abscess or a chronic sinus tract.
2
Microbiology of apical periodontitis
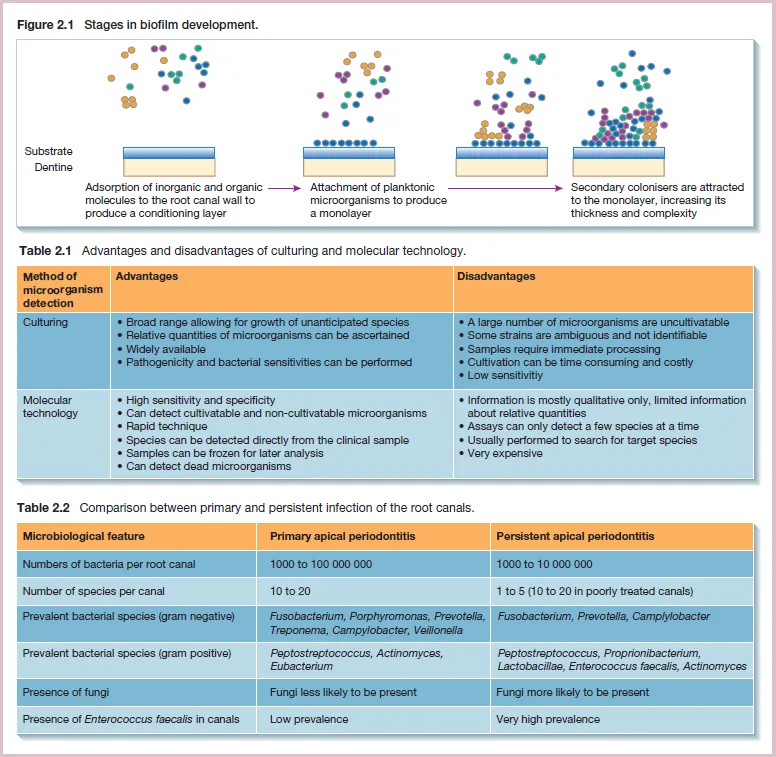
Which methods of sampling are used for...
Table of contents
- Cover
- More Details
- Title Page
- Copyright
- Dedications
- About the companion website
- Part 1 Disease processes in endodontology
- Part 2 Diagnosis
- Part 3 Endodontic therapy
- Part 4 Pain and pain management
- Part 5 Outcome of endodontic treatment
- Part 6 Endodontology and other aspects of dentistry
- Part 7 Trauma
- Part 8 Risk management
- Index
- End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Endodontology at a Glance by Alix Davies,Federico Foschi,Shanon Patel in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over one million books available in our catalogue for you to explore.