- English
- ePUB (mobile friendly)
- Available on iOS & Android
Emergency Nursing at a Glance
About this book
From the publishers of the market-leading at a Glance series comes a wide-ranging and succinct overview of the key concepts of emergency care. Emergency Nursing at a Glance uses the unique and highly visual at a Glance format to convey vital information quickly and efficiently, ensuring that nursing students have access to all the important topics they need for an emergency care placement. This highly visual, easy-to-read guide is the ideal companion for anyone entering fields involving urgent or unscheduled care.
•Includes all aspects of emergency care, including trauma, minor injury, triage processes, patient assessment, common emergency presentations, as well as legal, ethical and professional issues.
•Covers care of adults, children, and those with learning disabilities and mental health conditions
•Presented in the bestselling at a Glance format, with superb illustrations and a concise approach
Emergency Nursing at a Glance is an invaluable resource for nursing students, newly qualified nurses and other healthcare professionals working in emergency departments, urgent care centres, minor injury units and walk-in centres.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Part 1
Initial patient assessment
- 1 The context of emergency nursing
- 2 Pre-hospital care
- 3 Triage
- 4 The ‘ABCDE’ approach
- 5 Track and trigger systems
- 6 Pain
1
The context of emergency nursing
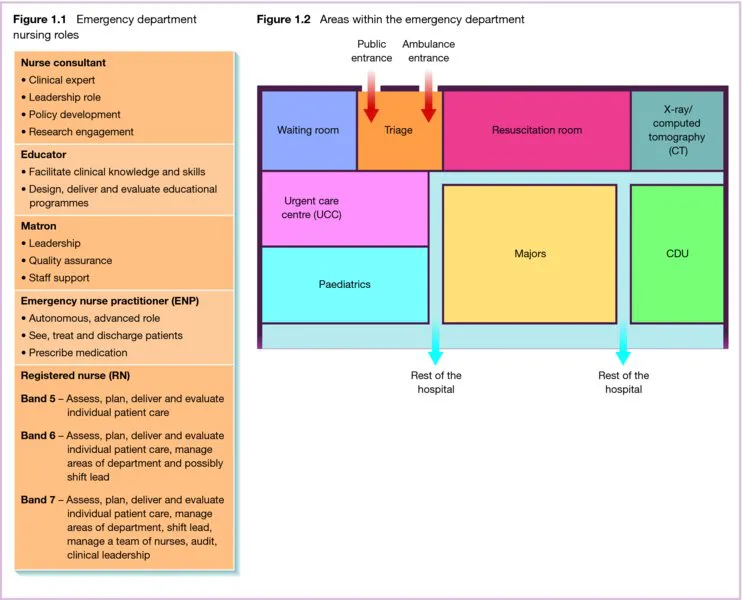
ED team
4-hour target
Areas within the ED
Triage
Resuscitation area
Majors
Minors/Urgent care centre (UCC)
Children
Observation area/Clinical decision unit (CDU)
Table of contents
- Cover
- Front matter
- Title page
- Copyright
- Contributors
- Preface
- Acknowledgements
- About the companion website
- Part 1 Initial patient assessment
- Part 2 Airway and breathing
- Part 3 Circulation
- Part 4 Disability
- Part 5 Emergency presentations and conditions
- Part 6 Poisoning and overdose
- Part 7 Infectious diseases
- Part 8 Vulnerable patient groups
- Part 9 Children in the emergency department
- Part 10 Minor injuries and conditions
- Part 11 Major Trauma
- Part 12 Patient transfer and end of life care
- Further reading/references
- Index
- EULA
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app