![]()
Chapter 1
How the NTSP resources were developed
These NTSP resources are for medical, nursing, allied health staff and students. There are resources for patients available separately.
This project started with a group of four Intensive Care Doctors working in Manchester, UK, who wanted to improve the management of patients with tracheostomies. We had identified recurrent themes common to tracheostomy and laryngectomy emergencies and recognised that in order to improve care, educational resources and innovative ways to teach them were urgently required. We initially sought the help of other colleagues in Critical Care, Anaesthesia, ENT surgery and maxillofacial surgery, forming a multi-disciplinary, multi-site working party to develop these resources. This group grew to incorporate input from nursing, physiotherapy and speech therapy colleagues, along with patients and patient groups and other medical and allied health professionals. A short video describing the origins of the project can be viewed at the url provided in the footnote.1
We have focused our attentions in two key areas: the emergency management algorithms and improving routine care by developing educational resources aimed at preventing neck-breathing patients developing life-threatening emergencies.
We developed and tested our emergency guidance with high-fidelity simulators using specific scenarios to ensure that nursing staff, doctors and allied health professionals could follow our algorithms. We have also introduced this guidance in a number of different trusts in the UK and developed the project incorporating multi-site, multi-speciality peer review and feedback.
The resources are supported by an extensive e-learning package, developed in partnership with the UK Department of Health's e-Learning for Healthcare project and the Royal College of Anaesthetist's e-Learning in Anaesthesia project. We have provided as much information as possible in video, diagram and schematic format, with many links from the text of this manual direct to YouTube videos and the resources of our website.2 This was in response to feedback received when we started to disseminate this information more widely. A lot of tracheostomy-related procedures are best learned when you can actually see someone doing it – either at the bedside locally, or via some of the videos we have provided. The resources in the manual have arisen from extensive collaboration between local, national and international stakeholder groups and have built on previously published guidelines, resources and expert opinion. We saw our role as putting together the individual pieces of the jigsaw that often existed in respect to specialised areas of tracheostomy and laryngectomy care.
The various resources have been peer reviewed by a number of different processes, including open peer review of draft resources posted on our website and the websites of a number of partner organisations. The emergency guidelines, algorithms, bedhead signs and supporting manuscript have been endorsed by the Difficult Airway Society, Intensive Care Society, the Royal College of Anaesthetists, ENT UK, British Association of Oral and Maxillofacial Surgeons, College of Emergency Medicine, Resuscitation Council UK, Royal College of Nursing, Royal College of Speech and Language Therapists, Association of Chartered Physiotherapists in Respiratory Care, National Association of Laryngectomy Clubs and the National Patient Safety Agency. There have also been contributions from The British Laryngological Association and the Faculty of Intensive Care Medicine. The NTSP manual has been reviewed by many of these groups, either formally or informally, and also revised by a multi-disciplinary NTSP editorial board. Finally, the e-Learning for Healthcare resources have been reviewed by e-Learning Anaesthesia at the Royal College of Anaesthetists.
Full details of the literature, review process and development of these guidelines are described in McGrath et al.'s (2012) manuscript3 in Anaesthesia.
![]()
Chapter 2
What is a tracheostomy? What is a laryngectomy?
What is a tracheostomy?
Tracheostomies are performed in head and neck surgical practice, with over 5000 procedures performed yearly in England. We estimate around 10 000–15 000 percutaneous tracheostomies are performed each year in England's critical care units, although the actual figure is currently unknown. Tracheostomies are also becoming more commonplace on the general wards of the hospital. This is partly due to pressures on intensive care beds and the increasing drive to de-escalate care quickly, along with increasing numbers of patients benefiting from temporary tracheostomies. These groups include those with chronic respiratory or neurological problems. Increasing numbers of patients with tracheostomies are being cared for on wards outside the specialist ward [typically ENT or maxillofacial wards, or sometimes neurosurgical or neurology wards] or critical care infrastructure.
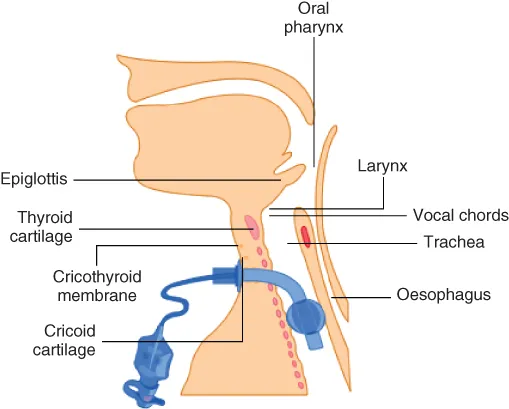
This has implications for the safety of patients who may be cared for on wards without the necessary competencies and experience to manage this challenging cohort and local measures need to be in place to ensure that safe routine and emergency care can be provided. This manual has evolved to provide information to those caring for patients with temporary or permanent tracheostomies, either regularly or occasionally. It aims to provide basic background information and the rationale for tracheostomy care (Figure 2.1).
What problems can occur with tracheostomies?
While tracheostomies are increasingly commonplace, patient safety incidents associated with their use are unfortunately increasing. Over 1700 incidents were reported to the NPSA between 1 January 2005 and 31 December 2008, including over 30 deaths. We know from research with the NPSA that when a clinical incident occurs relating to a tracheostomy, the chance of some harm occurring is between 60% and 70%, depending on the location in which that the patient is being cared for [see links to these abstracts for NPSA papers in Thomas and McGrath (2009) and McGrath and Thomas (2010)].
Incidents may be classified as
- incidents at the time of performing the tracheostomy (e.g. airway loss; damage to adjacent structures; bleeding);
- blockage or displacement of the tracheostomy tube after placement;
- equipment incidents (usually lack of equipment or inappropriate use);
- competency (skills and knowledge) incidents;
- infrastructure (staffing and location) incidents;
- late complications (e.g. tracheomalacia, stenosis, infection of stoma).
The majority of these incidents are due to the same recurring themes and the resources we have developed as part of this project are specifically aimed at addressing these.
There is more detail on tracheostomy and laryngectomy problems in the complication, red flags and emergency management section.
What is a laryngectomy?
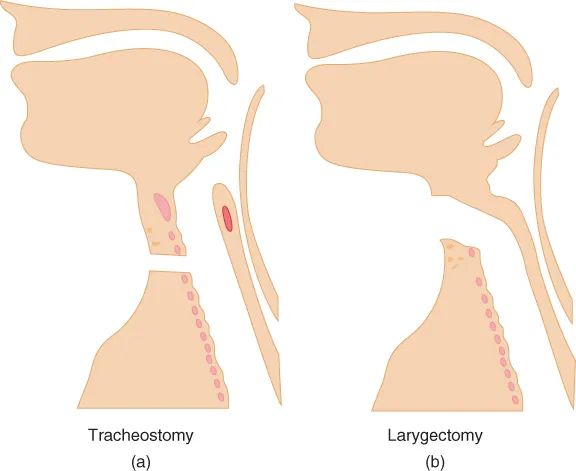
The larynx (voice box) can be involved in oral, pharyngeal or laryngeal carcinomas. These are usually squamous cell carcinomas and can be treated by radiotherapy and surgery, depending on the site and the general condition of the patient. Surgical resection of the tongue base or epiglottis may not necessarily involve removal of the larynx and is sometimes referred to as a supraglottic laryngectomy. It is sometimes possible to resect only one half of the larynx for localised disease with a hemilaryngectomy. However, if a total laryngectomy is required, this involves complete surgical removal of the larynx, which disconnects the upper airway (nose and mouth) from the lungs. This is a permanent and irreversible procedure (although partial laryngectomies are possible). The trachea is transected (cut) and then the open end is stitched onto the front of the neck. Once this has been performed, the patient will never be able to breathe or be oxygenated or ventilated through the upper airway again. An animation showing the difference between a tracheostomy and a laryngectomy1 can be found in the link provided in the footnote.
As shown in Figure 2.2, a tracheostomy still provides a potentially patent upper airway. Remember though that tracheostomies are often performed because of actual or anticipated difficulty with the upper airway, so upper airway patency cannot be guaranteed.
What problems can occur with laryngectomies?
The laryngectomy patient has had the normal upper airway humidification mechanisms bypassed, in the same way as a tracheostomy patient. They are at risk of blockage of the trachea with secretions or blood. The airway is often more secure than with a temporary tracheostomy, as the trachea is stitched onto the front of the neck. It can still become compromised, however, particularly within a few days of surgery. Laryngectomy stomas are usually simple open stomas without a tube inserted. There are a variety of covers, valves and humidification devices available, which can make distinguishing between a tracheostomy and laryngectomy very difficult. Tubes are sometimes inserted into laryngectomy stomas, especially when they have just been created; the patient needs invasive ventilation or requires repeated suctioning. Tracheostomy tubes are usually used, although specific laryngectomy tubes are available. The use of bedhead signs to alert staff that a patient does not have an upper airway is extremely useful, especially when the patient cannot tell you because of acute illness or not being able to talk following a laryngectomy.
One of the commonest problems with a laryngectomy, particularly in an emergency, is that responders fail to appreciate that the patient has actually had the larynx removed. It can be difficult to tell the difference at the bedside between a laryngectomy and a surgical tracheostomy, particularly close to major surgery. There are...