![]()
What is hypertrophic cardiomyopathy (HCM)
Cardiomyopathy is a general term describing any condition in which the heart muscle is structurally and functionally abnormal (the heart itself is, of course, a specialized type of muscle). While there are many types of cardiomyopathy (e.g., dilated, restrictive, and right ventricular), many of which are genetic and familial, we are concerned here with only hypertrophic cardiomyopathy (HCM).
HCM is a genetic disease affecting the heart muscle. The most consistent feature of HCM is excessive thickening (hypertrophy) of that portion of the heart known as the left ventricle. In quantitative terms, hypertrophy is usually defined as a wall thickness of 15 mm or more when measured by ultrasound (echocardiogram) or cardiac magnetic resonance imaging (MRI), but any wall thickness (including normal) is consistent with the presence of a gene causing HCM. The consequences of HCM to patients are related, in part or solely, to the abnormally thickened left ventricular heart muscle, which in turn is a consequence of the basic genetic defect. Hypertrophy may be widespread throughout the left ventricle, but may also be more limited in distribution, involving only very small portions of the wall; there is no single pattern of muscle thickening which is “typical” for HCM. The region of the left ventricle which is usually the site of the most prominent thickening is the ventricular septum, that is, that portion of muscle which separates the left and right ventricular cavities. These patterns of hypertrophy do not represent separate disease states, but are all part of the HCM spectrum.
The heart (specifically the left ventricle) may also thicken in other individuals who do not have HCM, either as a result of high blood pressure, obstructive heart valve disease, or even occasionally with prolonged and intense athletic training in certain sports. The type of hypertrophy of the left ventricle associated with high blood pressure is often referred to as secondary (i.e., a consequence of the increased blood pressure). In HCM, however, the muscular thickening of the heart wall is primary – that is, due to a genetic defect and not a reaction to other factors.
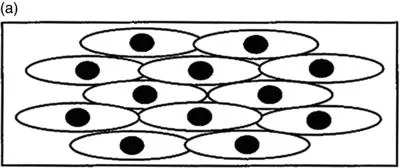
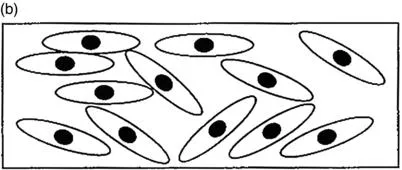
In addition, when the heart muscle of HCM is viewed under a light microscope, it usually shows several particular abnormalities, the most prominent of which is myocardial cell (myocyte) disarray or disorganization, in which the normal parallel alignment of heart muscle cells has been lost and many of the muscle cells are arranged in characteristically chaotic and disorganized patterns (Figure 1). It is likely that this cell disarray interferes with normal electrical transmission of impulses and predisposes some patients to irregularities of heart rhythm (and sudden death), as well as altering heart contraction. In addition, there are often collagen scars (i.e., areas of fibrosis of various size and extent within the left ventricular wall), which probably result from inadequate blood supply to the heart muscle.
- HCM is a common genetic cardiac disease causing the heart wall to thicken without enlarging the cavities.
- HCM is diverse in its presentation.
- Some people with thick hearts may not have HCM and instead the thickness may result from high blood pressure, valve disease, or prolonged athletic training.
Historical perspective and names
The first modern description of HCM was in 1958 by a British pathologist, Dr. Donald Teare, who likened the disease to a tumor of the heart. However, there is some evidence that HCM was initially recognized in the mid-1850s by German and French investigators. Nevertheless, over these many years, the condition has been known by a vast number of names. Indeed, this issue of nomenclature is often confusing to patients and even some physicians.
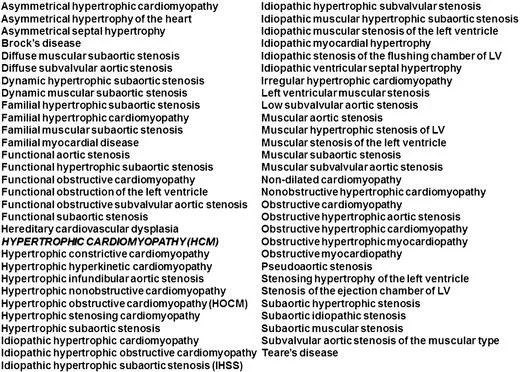
Remarkably, HCM has been given over 75 separate names by individual clinicians and scientists over the last 50 years (Figure 2). Literally, no other disease can make that claim. Why has this occurred? The principal reason for the proliferation of names undoubtedly has been the clinical heterogeneity and diversity with which HCM is expressed, a major point in ultimately understanding this disease. Also, since very few cardiologists have treated large numbers of patients with HCM, they often came to regard the overall disease based solely on their personal (and sometimes limited) experiences.
Many of the alternate names for HCM emphasize obstruction to left ventricular outflow, which is a highly visible feature of the disease. Obstruction is probably present under resting conditions in just 25% of all patients; however, about 70% of all HCM patients have the capacity to generate obstruction, either at rest or (if not present at rest) when provoked by physiologic exercise. Therefore, names for this disease in the past have included idiopathic hypertrophic subaortic (stenosis) (IHSS), which was the first popular term used in the United States (“stenosis” means obstruction). The same can be said for hypertrophic obstructive cardiomyopathy (HOCM), which is still widely used in the United Kingdom. Indeed, you may well hear your disease referred to by more than the currently accepted designation – HCM.
Indeed, virtually all HCM experts and other cardiovascular specialists now regard HCM as the single best name for the broad disease spectrum. The term combines hypertrophy (which is the diagnostic marker in most patients) with the fact that this disease is a cardiomyopathy (or heart muscle disorder), and furthermore excludes specific reference to obstruction (which is not present in all patients). Therefore, the terms “HCM with obstruction” or “HCM without obstruction” are preferred.
HCM is a genetic disease based on the recognition 20 years ago that it is caused by mutations in genes coding proteins in the heart muscle. It is also a familial disease because it is transmitted to every generation as a dominant trait (i.e., about 50% of each generation are at risk). HCM is usually inherited, but there is also a phenomenon of de novo mutation when the disease (and mutation) appears for the first time in a family. It is probably not proper to consider HCM a congenital heart disease since it is only the disease-causing mutation which is always present from birth.
- HCM has had many names in the past.
- Hypertrophic cardiomyopathy or “HCM” is the preferred terminology.
How common is HCM?
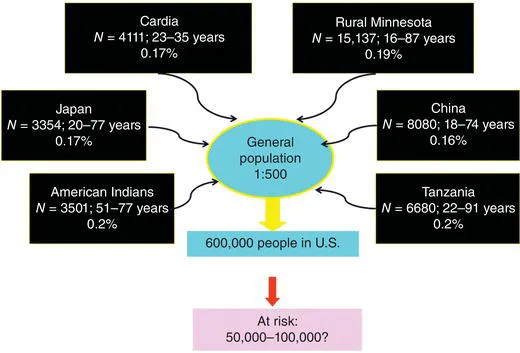
HCM has had a misleading reputation as a rare disease. It is global in distribution, reported from all continents and more than 50 countries. However, a number of recent population studies from the United States and elsewhere in the world show that HCM is a much more common disease than previously regarded. It is now estimated that at least about 1 in 500 individuals within the general population are affected by this disease, equivalent to about 750,000 Americans (Figure 3). HCM is truly a global disease and these prevalence figures come from populations as diverse as the United States, Japan, Africa, and China. These figures relate to adults in whom the disease is recognized by echocardiography (i.e., by visualizing the thickening of the left ventricular wall). However, many other children and adults could carry a mutant gene for HCM and not be easily detectable by echocardiography or not come to clinical recognition for a variety of reasons (including absence of a heart murmur and obstruction), and therefore may be completely unaware of their diagnosis. Indeed, the 1 in 500 prevalence figure is likely to be an underestimate given the large number of genetically affected individuals in HCM families with little or no overt clinical evidence of the disease.
Indeed, the currently recognized HCM patient population has been likened to the “tip of the iceberg,” with most affected patients undiagnosed and “below the surface” (Figure 4). This helps explain why HCM seems so uncommon in cardiology practice, that is, why cardiologists so often tell HCM patients that they only occasionally see this condition.
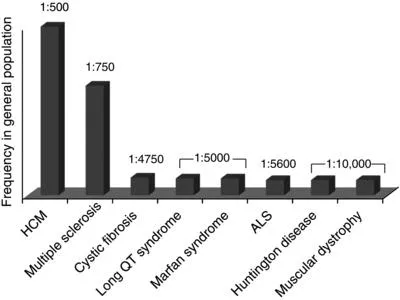
The large number of names used to describe HCM may be one factor responsible for the perceived low visibility of HCM in the public sector relative to other less common diseases. In fact, HCM is much more common, and has more impact on the public health, than more visible noncardiac conditions such as cystic fibrosis, multiple sclerosis, muscular dystrophy, and amyotrophic lateral sclerosis (ALS; Lou Gehrig disease), or cardiovascular diseases such as Marfan syndrome (Figure 5). These other conditions are truly rare, occurring in only 1:10,000 or less of the general population while HCM is the most common genetic heart disease and most frequent cause of sudden death in the young – occurring in 1:500 people (Figure 5).
HCM occurs throughout the world (Figure 6), with most of the scientific interest and reports from North America (United States and Canada), the Far East (Japan, China, Australia), and Europe (United Kingdom, Italy, France, Germany, Switzerland), although there is increasing attention to HCM in Brazil, Argentina, Chile, Israel, and New Zealand. HCM appears to be remarkably similar with regard to its clinical presentation, heart structure, clinical course, and prognosis in patients from these diverse areas of the world. One relatively minor exception is the apical form of HCM with wall thickening localized to the tip [apex] of the left ventricle, always without obstruction, which seems to be more common in Japan – a distinction which could reflect unique racial, ethnic, and/or environmental factors. This structural form is not a separate disease entity and also occurs in 3% of US (non-Asian) patients, due to the same mutations that cause other forms of HCM.
- HCM is common; 1 in 500 people in the general population have HCM but many more may carry the gene and not be aware.
- HCM affects people of many nationalities, both genders, and all ages.
What is the cause of HCM?
As emphasized earlier, HCM is a genetically transmitted and usually familial condition. The pattern of inheritance of HCM is known as autosomal-dominant, which means that the disease (and the mutant gene) occurs in about 50% of the relatives in each consecutive generation (Figure 7). Therefore, the likelihood of an affected parent transmitting the abnormal gene to their child is statistically about one in two. However, autosomal-dominant inheritance does not necessarily mean that in each family if there are four offspring, two must be affected – o...