eBook - ePub
Mood Disorders
Practical Issues in Diagnosis and Management
Ather Muneer
This is a test
- 212 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Mood Disorders
Practical Issues in Diagnosis and Management
Ather Muneer
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Mood Disorders: Practical Issues in Diagnosis and Management provides cutting edge knowledge about the diagnosis and treatment of principal mood disorders, namely major depressive disorder and bipolar disorder. Covering diagnosis, differentiating features, and illness course and trajectories of principal mood disorders, Dr. Ather Muneer provides essential information in a succinct and practical manner, while highlighting significant new findings in the area. This book will help a broad range of mental health professionals better treat the millions ofpeople withmood disorders across the globe.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Mood Disorders est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Mood Disorders par Ather Muneer en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Psychiatry & Mental Health. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
1Major Depressive Disorder and Bipolar Disorder
Introduction
According to the Diagnostic and Statistical Manual of Mental Disorders – 5th Edition (DSM-5) major mood disorders are classified into major depressive disorder (MDD) and bipolar disorder (BD). More than a century ago, the German psychiatrist Emil Kraepelin categorized major mental disorders into “manic depressive insanity” and “dementia praecox”. The former was re-conceptualized as a recurrent illness exemplified by repeated depressive and manic episodes while the latter was replaced by “schizophrenia”, a word coined by the Swiss psychologist Eugene Bleuler and typified as a non-affective psychosis epitomized by delusions, hallucinations, blunting of affect and loss of motivation.1 In the current rendition of DSM-5, MDD and BD are described under separate rubrics as these mood disorders are presently considered to have distinct etiology, pathogenesis, course and therapeutic connotations.
Major mood disorders are highly prevalent conditions affecting up to 20% of the general population.2 Individuals of both sexes are afflicted, onset is usually in teenage years or early adulthood and the disorders follow a relapsing and remitting course throughout life. All the current treatments are palliative rather than curative in nature, and while the modern psychopharmacological agents have improved safety and efficacy, these still impose a huge burden with respect to adverse effects. Consequently, compliance is low and relapse rate is high with resultant impairment in the biopsychosocial realms of functioning.3 Affective disorders are a leading cause of morbidity and mortality, since these are regarded as systemic ailments and are very often associated with such comorbid conditions as diabetes mellitus, cardiovascular diseases, autoimmune disorders and endocrine disturbances.4 The majority of people who commit suicide have an underlying mood disorder, and new data suggest that the incidence of this condition is on the rise across the world.5 Because of these reasons World Health Organization statistics show that mood disorders are an important source of disability and death globally.6 Therefore, in the light of such considerations it is crucial that physicians in general and mental health professionals in particular, have an adequate understanding of these very common psychiatric conditions.
Signs and Symptoms
Historical development in the nosology of mood disorders has led to their categorization into unipolar depression and BD. Essentially these are distinct conditions with different genetic underpinnings and disparate illness trajectory, progression and outcome. In essence, MDD is typified by recurrent depressive exacerbations without a lifetime history of hypomanic or manic episodes, whereas BD patients fluctuate between the opposite mood states of depression and mania.7
Major Depressive Episode
A major depressive episode (MDE) is signified by the presence of low mood and loss of pleasure in day-to-day activities, aptly termed anhedonia. The latter represents a distinct emotional tone in the patients, wherein they lose interest in the usual activities and no longer experience pleasure in things they previously found enjoyable. The cognitive process in MDE is exemplified by excessive guilt and self-blame, thoughts of helplessness and hopelessness and suicidal ideation. Disruption in the circadian rhythm is evident as sleep disturbance, with early morning wakening characterizing the more severe, melancholic form of MDD. There is usually decreased appetite and weight loss, but patients with “atypical depression” can have reverse vegetative disturbance with hypersomnia, increased food intake and weight gain. Subjects who have MDEs experience excessive mental and physical fatigue, loss of energy and tiredness and also complain of difficulty in concentration and indecisiveness. Further, they may show psychomotor retardation or agitation. Recurrent suicidal ideation and psychomotor agitation accompanying a low mood predisposes MDD patients to self-harm and attempted or completed suicide.8 While the duration criteria stipulate a minimum period of two weeks, in the usual scenario patients are symptomatic for months before they seek medical help. As can be construed from the abovementioned facts, an MDE is a serious ailment which can prove fatal if there is delay in diagnosis and treatment. The vast majority of patients with MDD follow a relapsing and remitting course, and while it is possible to have a single lifetime MDE, this is the exception rather than the rule.9
Manic Episode
A manic episode is the sine qua non of BD and patients typically present with elevated or expansive mood. They have raised self-esteem and express grandiose ideas, which in the case of psychotic mania can be of delusional intensity. Subjectively, patients experience racing thoughts and objectively this is manifested as pressure of speech and flight of ideas. They have boosted energy levels and show increase in goal-directed activities; coupled with this is a decreased need for sleep. In severe mania, the patient is on the go most of the time, has boundless energy and feels rested after only a few hours of sleep. These subjects exhibit overindulgence in pleasurable activities and become part of risky ventures with high potential for harmful social consequences. Some examples are buying sprees, sexual indiscretions, and alcohol and substance abuse. A manic patient requires urgent treatment and is often in need of psychiatric hospitalization. Whereas the duration criteria stipulate a period of disturbance spanning one week, if hospitalization is mandated then a manic episode can be diagnosed with any period of mood disturbance.10 The core symptoms of a hypomanic episode are essentially analogous to a manic episode, with the caveat that severe psychosocial disruption is not evident and emergency hospitalization is not needed.11 Only four days of mood disturbance is sufficient to diagnose a hypomanic episode and, while the disorder is subtle in presentation, it is often part of chronic affective instability in bipolar spectrum disorders.
Mixed States
Mood symptoms can manifest in numerous ways and typical presentations are seen in only a minority of patients. A common clinical occurrence is the presence of mixed affective states, which can afflict people with both MDD and BD. The current conceptualization of mixed states posits that symptoms of opposite mood polarity are attendant in patients with major mood disorders. It is estimated that up to 40% of bipolar patients may be afflicted in this manner, while concurrent presence of hypomanic or manic symptoms in MDD is being increasingly recognized.12 In essence, this implies that patients with manic or hypomanic episodes have coexisting depressive symptoms and vice versa. The clinical significance of mixed states is manifold. Firstly, the clinician should be cognizant of their occurrence and be on the lookout for the presence of mixed affective manifestations in patients with mood disorders. Secondly, it should be realized that repeated episodes of similar polarity occur, such that patients with mixed episodes tend to have the same exacerbations in the course of their illness. Thirdly, mixed episodes signify a more severe illness trajectory marked by treatment resistance, greater neuropsychiatric comorbidities and higher risk of suicide. Lastly, polypharmacy is the rule rather than the exception in the management of these cases and there is consequential patient noncompliance from medication adverse effects.13
Figure 1.1 is an illustrative rendition of the different mood states as envisaged in DSM-5. Table 1.1 recapitulates the main affective states as encountered in discrete mood episodes.
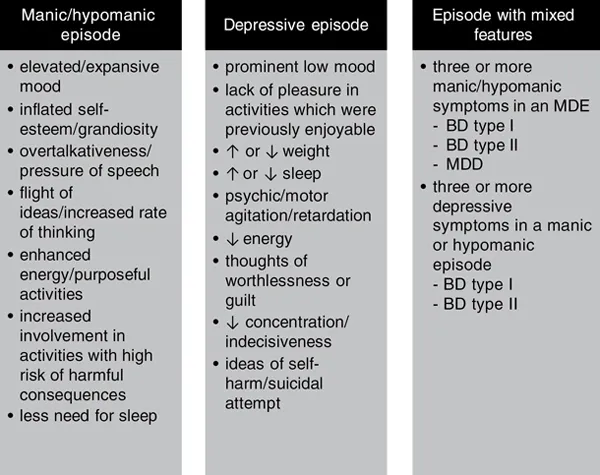
Figure 1.1Diagnostic criteria for manic, depressive and mixed states according to DSM-5
As opposed to previous editions, in DSM-5 the specifier “with mixed features” is used for manic, hypomanic or depressive episodes in bipolar spectrum and major depressive disorders. The term “mixed episode” employed in the setting of BD type I has been discontinued in DSM-5.
BD – bipolar disorder; MDD – major depressive disorder; MDE – major depressive episode
Table 1.1Diagnostic features of different affective states according to DSM-5
| Symptom domain | Hypo/manic episode | Depressive episode | Episode with mixed features |
| Subjective mood | Elated | Depressed | Varies |
| Hedonic tone | ↑involvement in pleasurable activities | Anhedonia | Mixture of both |
| Thought content | Grandiose | Worthlessness/guilt | Varies |
| Talk | ↑in rate, rhythm and volume | ↓in rate, rhythm and volume | Incongruent e.g. depressed mood with pressure of speech |
| Behavior | Risky behaviors | Suicidal acts | Contrasting e.g. elevated mood with suicidal ideation |
| Energy | ↑ | ↓ | ↑↓ |
| Sleep | ↓need for sleep | Early morning wakening | Severely disturbed |
| Thoughts | Racing thoughts | Difficulty in thinking/concentration | Incongruent e.g. depressed mood with racing thoughts |
| Appetite/weight | Disrupted meal schedule | ↓ | Severe disruption |
| Duration | Hypomania – 4 days; mania – 7 days | 14 days | Duration criteria no longer apply |
| Minimum criteria for mixed episode | Three depressive features in hypomanic or manic episode | Three manic features in a depressive episode | Mixed hypomania – BD type I or II Mixed mania – BD type I MDE with mixed features – BD type I or II/MDD |
| Functioning | Hypomania – impaired but does not require hospitalization Mania – severely impaired/may need hospitalization | Impaired according to degree – mild/moderate/severe | Varies according to diagnosis |
BD – bipolar disorder; MDD – major depressive disorder; MDE – major depressive episode
Diagnosis of Mood Diso...
Table des matières
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- List of Figures
- List of Tables
- 1 Major Depressive Disorder and Bipolar Disorder
- 2 Major Mood Disorders: Differentiating Features
- 3 Comorbidity in Mood Disorders
- 4 The Role of Epigenetics
- 5 Neurobiology of Mood Disorders: The Circadian Connection
- 6 Pathogenesis of Mood Disorders: The Neuroinflammatory Hypothesis
- 7 Staging and Neuroprogression of Mood Disorders
- 8 The Management of Treatment-Resistant Depression: Monoamines and Beyond
- 9 Depressive Phase of Bipolar Disorder: Treatment Recommendations
- 10 Manic Phase of Bipolar Disorder: Treatment Recommendations
- 11 Non-Pharmacological Treatments for Mood Disorders
- Index
Normes de citation pour Mood Disorders
APA 6 Citation
Muneer, A. (2018). Mood Disorders (1st ed.). Taylor and Francis. Retrieved from https://www.perlego.com/book/1580270/mood-disorders-practical-issues-in-diagnosis-and-management-pdf (Original work published 2018)
Chicago Citation
Muneer, Ather. (2018) 2018. Mood Disorders. 1st ed. Taylor and Francis. https://www.perlego.com/book/1580270/mood-disorders-practical-issues-in-diagnosis-and-management-pdf.
Harvard Citation
Muneer, A. (2018) Mood Disorders. 1st edn. Taylor and Francis. Available at: https://www.perlego.com/book/1580270/mood-disorders-practical-issues-in-diagnosis-and-management-pdf (Accessed: 14 October 2022).
MLA 7 Citation
Muneer, Ather. Mood Disorders. 1st ed. Taylor and Francis, 2018. Web. 14 Oct. 2022.